KEYWORDS
Chlamydia, Chlamydophila, pneumonia, polymerase chain reaction, psittacosis
INTRODUCTION
Chlamydia psittaci is an intra-cellular Gram-negative bacterium which may cause zoonotic pneumonia in humans.1 Usually, transmission occurs through inhalation of aerosols from contaminated bird substances such as droppings, plumage, or tissue.2 Few studies have evaluated the incidence of C. psittaci in hospitalised community-acquired pneumonia (CAP); reported incidence rates range from 0% in Korea in the years 1999-2000,3 to 0.002% in Australia in 2004-2006,4 0.004% in Canada in 1996-1997,5 and 0.36% in Spain in 1996-1997.6 These rates are probably an underestimation of the true incidence since even brief exposure can lead to systemic infection7 and testing for C. psittaci is often only included in the diagnostic algorithm if the clinician is aware of contact with birds in the patient’s history. Although the disease is notifiable to the public health authorities in the Netherlands, detection of psittacosis is frequently not incorporated in routine microbiological diagnostic panels for pneumonia. Since standard β-lactam based antibiotic therapy is not adequate for the treatment of C. psittaci, this might lead to progression of infection.
Psittacosis can be diagnosed by culture, but C. psittaci is difficult to grow. Furthermore, biosafety level three facilities and cell cultures are required which are not available in most medical microbiology laboratories. Currently, polymerase chain reaction (PCR) of sputum or bronchial secretions and serology are the cornerstones of microbiological diagnosis. All aforementioned studies on psittacosis incidence used only serological diagnostic methods such as complement fixation test (CFT) and micro-immunofluorescence. Due to the retrospective aspect and cross-reactivity with other Chlamydia species, detection by serology is not optimal. If sputum is available, PCR is a method with fast results and lacking genus broad cross-reactivity.8 The availability of sputum enables genotyping of the strain. A recent study from Germany reported a C. psittaci incidence of 2.1% in CAP, based on C. psittaci PCR on pharyngeal swabs in all CAP patients who presented to the emergency department.9
We analysed a cohort of 304 patients hospitalised with CAP in which PCR and CFT for psittacosis diagnosis were incorporated in the diagnostic algorithm. We also analysed whether specific clinical parameters were associated with CAP caused by C. psittaci. Furthermore, we evaluated the contribution of serology to the diagnosis of psittacosis by PCR.
MATERIALS AND METHODS
Study design and patients
Our analyses were performed in all patients in whom a sputum or bronchoalveolar lavage sample was available in a cohort of 304 hospitalised patients with CAP who participated in a randomised clinical trial conducted in the Netherlands from November 2007 until September 2010 (NCT00471640). The original trial investigated the adjunctive treatment of dexamethasone 5 mg given intravenously. Detailed inclusion and exclusion criteria are described elsewhere.10 In summary, patients with CAP admitted to the St. Antonius Hospital (Nieuwegein, the Netherlands) or the Gelderse Vallei Hospital (Ede, the Netherlands) were included. Pneumonia was defined as a new pulmonary infiltrate on chest radiograph, in combination with at least two of the following criteria: cough, sputum production, temperature > 38.0 °C or < 35.0 °C, auscultatory findings consistent with pneumonia, C-reactive protein concentration > 15 mg/l, and white blood cell count > 10 x 109 cells/l or < 4 x 109 cells/l or > 10% of rods in leukocyte differentiation. Patients who were immunocompromised, who were admitted to the intensive care unit immediately, or who received immunosuppressive therapy were excluded. The study was approved by the local Medical Ethics Committees of both hospitals and all patients gave written informed consent.
Psittacosis diagnosis
Sputum or bronchoalveolar lavage was analysed with C. psittaci specific real-time PCR.11 Furthermore, acute-phase serum and convalescent serum samples were analysed for the presence of antibodies against Chlamydia species, with CFT using a Chlamydia-specific lipopolysaccharide (Virion-Serion, Ruschlikon, Switzerland). The interval between the first (day of admission) and second serum sample was at least ten days with a maximum of 120 days. A fourfold or greater rise of the antibody titre in the convalescent versus the acute-phase serum was considered indicative for a recent Chlamydia infection (sequence 1: < 4, 4, 8, 16, etc. or 1: < 10, 10, 20, 40, etc.). Sera of patients with a positive psittacosis PCR or CFT result were tested with micro-immunofluorescence (Focus Diagnostics, United States of America), using the same criteria for a rise in antibody titre that were used for CFT (sequence 1: < 16, 16, 32, 64, etc.). The case criteria for a diagnosis of psittacosis was a positive PCR or a fourfold rise of antibody titre in CFT confirmed by micro-immunofluorescence. Stored sputum samples were genotyped by partial ompA gene sequencing.12
Diagnosis of other respiratory pathogens
Two sets of separate blood samples and sputum samples were cultured. Urine antigen tests were performed for the detection of Streptococcus pneumoniae and Legionella pneumophila serogroup 1. Real-time PCRs on sputum were also performed to detect Legionella species, Mycoplasma pneumoniae and Coxiella burnetii. Moreover, St. Antonius Hospital samples were also tested for C. pneumoniae until November 2008. Acute versus convalescent serological testing was performed for antibodies to M. pneumoniae, C. burnetii and respiratory viruses (adenovirus, influenza virus A and B, parainfluenza virus 1, 2 and 3, and the respiratory syncytial virus). Pharyngeal swabs were taken for PCR to detect (para)-influenza virus, adenovirus and respiratory syncytial virus.
Clinical parameters and outcome
Clinical and laboratory parameters (table 1) were documented. For patients in whom information on bird contact was not available in the admission documents, the Dutch notification database of the Centre for Infectious Disease Control of reported psittacosis patients was checked for information on this subject.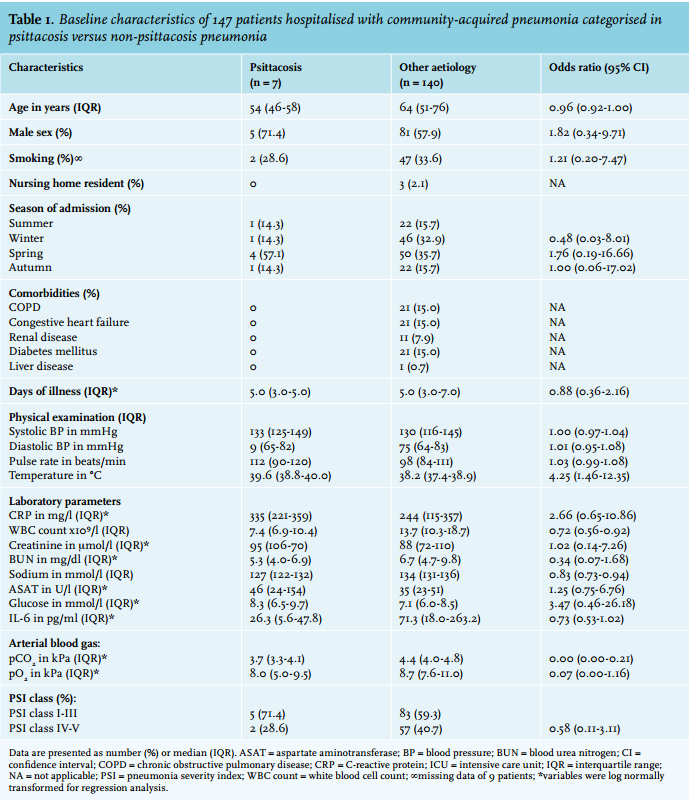
Statistical analyses
Overall, descriptives were stated as number (%) or median (interquartile range (IQR)). Patient characteristics between psittacosis patients and other aetiology were compared using Chi-square test, Fisher’s exact test, or Mann-Whitney U test, where appropriate. For this analysis, a p-value < 0.002 was considered significant, using the Bonferroni correction for multiple testing with 26 variables. To identify variables predicting psittacosis, logistic regression analysis was conducted in a univariate model. Variables which were not normally distributed were log-normally transformed to improve distribution. A multivariate analysis was not possible due to the small number of psittacosis patients. Data were analysed with SPSS statistical software for Windows, version 22.0.
RESULTS
Psittacosis diagnosis
In total, 304 CAP patients were enrolled in the original trial. Sputum was available in 154/304 patients for analysis with C. psittaci PCR. In seven patients the PCR reaction of sputum was inhibited. Therefore, 147/304 (48.4%) patients were eligible for further analysis, of which 77 patients received dexamethasone and 70 patients placebo in the original study. Of the 147 patients, six (4.1%) patients were diagnosed with psittacosis based on a positive PCR result. In 119/147 (81.0%) patients serological analysis for the presence of Chlamydia antibodies by CFT was performed as well. In nine patients, serum was positive on CFT. A confirmation with micro-immunofluorescence was positive in five out of nine patients, and four of these five were also positive on PCR. One PCR-positive patient was seronegative and one was sero-inconclusive. Based on our diagnostic criteria, we considered the one patient who was PCR negative but CFT and micro-immunofluorescence positive to be positive for psittacosis. In total, 7/147 (4.8%) patients were diagnosed with psittacosis based on PCR and serology results. Table 2 shows an overview of the test results. No other pathogens were detected in these seven patients. None of these patients were known to be involved in an outbreak. In three of six patients, sputum was available in storage for genotyping; two patients had genotype A, one patient genotype B.
In our cohort, most CAPs were caused by S. pneumoniae (38/147, 25.9%), followed by C. burnetii (12/147, 8.2%).10 The latter was high due to a national outbreak of Q fever.13Haemophilus influenzae was detected in six patients and Legionella species in five patients. In the 47 patients in whom Chlamydia pneumoniae PCR was performed, no positive results were found.
Of the 157/304 patients in whom no sputum was available for PCR, paired CFT was performed in 93 (59.2%) patients. Of these patients, three were positive on CFT, but specificity for C. psittaci was not confirmed by micro-immunofluorescence.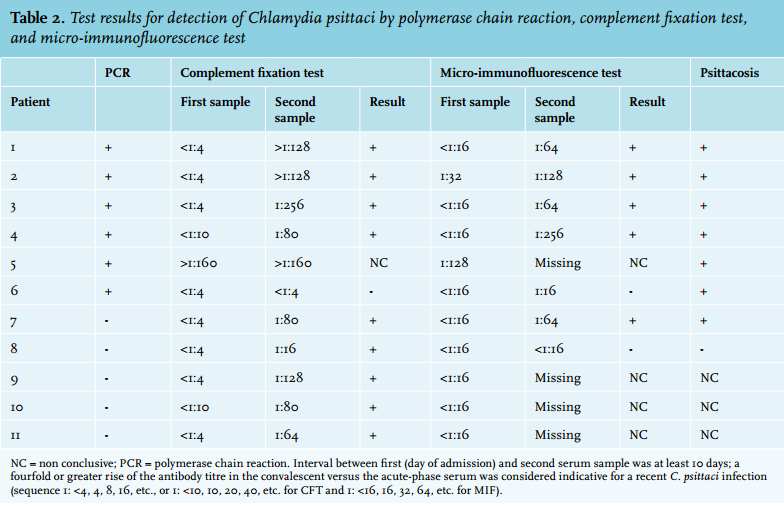
Description of psittacosis patients
Median age of the seven patients with a C. psittaci CAP was 54 years (IQR 46-58) and 71.4% were male. The median interval between onset of disease and admission to hospital in patients with psittacosis was 5.0 days (IQR 3.0-5.0 days).
Of the seven patients, five patients initially reported a positive history of bird contact, one a negative history, and for one patient history was not documented in the medical record. For this patient information on bird contact could be found in the Dutch notification database: a dead bird in the garden was reported. Table 3 shows an overview of clinical parameters of the seven psittacosis patients.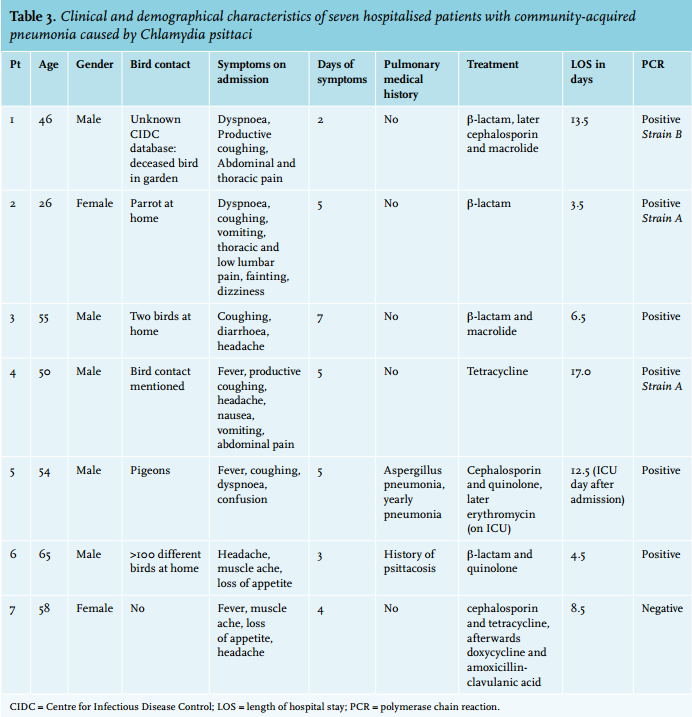
Characteristics of C. psittaci versus other pathogens
Baseline characteristics of the seven psittacosis patients were compared with the 140 CAP patients with other or unknown aetiology (table 1). There were no significant clinical or demographical differences between these two aetiological groups. Psittacosis patients had a higher median temperature (39.6 °C, IQR 38.8-40.0 vs. 38.2 °C, IQR 37.4-38.9) but lower white blood cell count (7.4 x109/l, IQR 6.9-10.4 vs. 13.7 x109/l, IQR 10.3-18.7) on admission, with ORs of 4.25 (95% CI 1.46-12.35) and 0.72 (95% CI 0.56-0.92), respectively. All odds ratios with 95% confidence intervals can be found in table 1.
Therapy
In five patients antibiotics adequate for psittacosis treatment were started in the emergency department (tetracycline, macrolide or quinolone antibiotics). In one patient adequate treatment was started later during admission based on a positive C. psittaci PCR. One patient was treated with β-lactam only. Length of stay did not differ between these two patients and the five patients who immediately received antibiotics regarded as adequate for the treatment for psittacosis. No patients died during the hospital stay.
DISCUSSION
In this study, PCR to detect C. psittaci was performed in all CAP patients for whom sputum was available. We found a much higher incidence of psittacosis (4.8%) than previously reported.
In most studies on CAP, psittacosis diagnostics are performed with serological tests only and no PCR.14 A recent study on aetiology in patients hospitalised with CAP in the United States did not perform C. psittaci diagnostics at all.15 A recent study from Germany did perform Chlamydia species PCR on pharyngeal swab specimens in all CAP patients presenting to the emergency department, and found an incidence of 2.1% for C. psittaci. 9 PCR leads to a quick diagnosis and lacks broad genus cross-reactivity.16 Furthermore, C. psittaci sputum strains can be genotyped, which is relevant for public health notification and source detection and control. However, sputum or bronchial alveolar lavage to perform a PCR are not always available. In these cases, serology can be informative. Moreover, in our study, one patient with a negative PCR had a positive CFT confirmed by micro-immunofluorescence. Including only patients in whom both PCR and serology were performed, the incidence of C. psittaci would be even higher in this study: 7/119 (5.8%). In this small population, we cannot explain why some patients were PCR positive and serology negative and vice versa. Serology does have the disadvantage of cross-reactivity with other Chlamydia strains. Furthermore, to confirm psittacosis two serum samples have to be drawn with an interval of at least ten days to detect a fourfold increase in antibody titre. Therefore, serology can only be used to diagnose psittacosis in retrospect and is mainly of additional value to optimise epidemiological investigations. Figure 1 shows reported psittacosis in the Netherlands in the period of study inclusion, based on the National Notification Database of the Centre for Infectious Disease Control. Nationally, this figure shows more psittacosis diagnosed serologically than by PCR. Regionally, in the areas where the study was conducted (in the centre of the Netherlands) and consequently psittacosis PCR was performed more routinely, the number of cases of PCR-confirmed psittacosis was higher compared with other areas. However, information on the number of PCRs and serology tests performed per region is unknown. The high number of reported psittacosis in the south-east area was mainly due to an outbreak of psittacosis after a bird fair in November 2007.17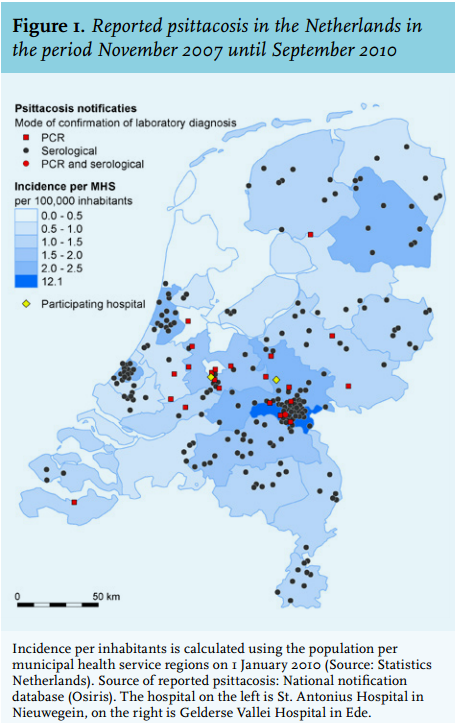
We addressed the question whether we could identify clinical parameters that discriminate psittacosis from CAPs caused by other pathogens. Due to the small sample size, the power of the statistical analysis was limited. The white blood cell count was almost normal in psittacosis patients, a finding consistent with a study on 135 serologyconfirmed psittacosis cases.18 Since elevated white blood cell count was one of the inclusion criteria of the original clinical trial, this could mean that psittacosis patients were less likely to be included and the real psittacosis incidence is even higher. In accordance with a study on the differences between C. psittaci and L. pneumophila in patients admitted to the ICU, patients with psittacosis seemed to have less comorbidities compared with those with CAP with other aetiologies, although this difference was not significant in our study.19 Further research with larger groups of psittacosis patients is needed to establish whether psittacosis can be identified as a separate clinical entity. This lack of specific alerting symptoms implies that doctors should be aware of the possibility of psittacosis in any case of CAP. In our study, one patient was treated with a β-lactam antibiotic only. This antibiotic is not recommended for the treatment of psittacosis, because C. psittaci lacks peptidoglycan. Either β-lactam antibiotics are also somewhat effective in psittacosis or the patient recovered due to the natural course of the disease.
Some limitations of the study must be mentioned. First, as mentioned previously, the number of psittacosis cases is small which limits statistical analysis. Second, since only two hospitals participated in this study it is unknown whether the results can be generalised. Third, CFT detects antibodies to Chlamydia species, but is not specific for C. psittaci due to cross-reactivity between the different Chlamydia species. Therefore, we performed micro-immunofluorescence to confirm the specificity of CFT results. It is assumed that micro-immunofluorescence does have species specificity. Finally, we included only patients in whom sputum was available for PCR diagnostics, which was 48.4% of the total CAP cohort. In the non-sputum group in whom serological analysis was performed, we found no evidence of an excess of psittacosis. On the contrary, there were less CFT/ micro-immunofluorescence serologically positive patients in the non-sputum group than expected: 0/94 in the non-sputum group compared with 5/119 in the sputum group (p=0.07). In the literature, there is no evidence that patients with psittacosis produce more sputum compared with CAPs with other aetiology.
In conclusion, in these two Dutch hospitals, where psittacosis PCR was performed if sputum samples were available, C. psittaci was more common as CAP-causing pathogen than previously reported. C. psittaci PCR is a fast method and sputum availability allows genotyping. Serology can be added to optimise epidemiological investigations.
ACKNOWLEDGEMENTS
We would like to thank Tjaco Ossewaarde (Department of Microbiology, Maasstad Hospital, Rotterdam, the Netherlands) for performing the micro-immunofluorescence assays. Furthermore, we would like to thank Ben Bom (National Institute for Public Health and the Environment, Bilthoven, the Netherlands) for compiling the map of reported psittacosis in the Netherlands.
DISCLOSURES
Willem Jan Bos received a grant during the conduct of the study from an individual person who supported the hospital research fund for research on CAP. No other grant support was received. The authors declare no conflict of interests.
REFERENCES