KEYWORDS
Doppler, follow-up, meld, survival, TIPS
INTRODUCTION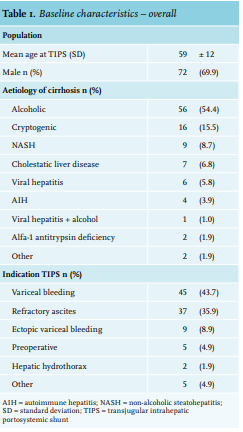
Liver cirrhosis represents the late stage of chronic liver disease and is associated with portal hypertension (PH). Most frequent complications of portal hypertension are bleeding of oesophageal or gastric varices, (refractory) ascites, and hepatic encephalopathy (HE). Placement of a transjugular intrahepatic portosystemic shunt (TIPS) is a highly effective intervention to reduce the portal pressure and to prevent rebleeding or treat refractory ascites.1 Since the introduction of polyfluor-ethylene (PTFE)-covered stents, patency has increased and the rates of stent thrombosis and in-stent stenosis have decreased drastically.2,3 Still, post-TIPS HE is a common (15-54%) complication that requires attention.4,5 This complication can be treated in 95% of the cases with drug therapy.6 However, patients often need hospital admission to undergo treatment.
There are few well-established prognostic markers that predict outcome after TIPS placement. The Model for End-stage Liver Disease (MELD) was initially developed to differentiate between patients who might benefit from TIPS and those who might not.7 However, MELD does not predict post-TIPS complications like the development of HE. Furthermore, there is no consensus regarding follow-up after TIPS placement. Currently, TIPS patients stay under close surveillance in most centres to monitor patency of the shunt with Doppler ultrasound (US) with assessment of blood flow through the shunt. American Association for the Study of Liver Diseases (AASLD) guidelines advise hospitals to have an established program for surveillance, but no specific intervals are suggested.6 At our institution, patients undergo Doppler US at day 5-7 after TIPS placement, followed by Doppler US at 3, 6, and 12 months, and subsequently every 12 months. The hepatologist sees the patient one month after TIPS placement to start lowering diuretics, and after each Doppler US study. The aim of this study was to assess the indications, survival, clinical outcome and yield, and usefulness of Doppler ultrasound for predicting TIPS failure at 3, 6, and 12 months after PTFE-covered TIPS placement in a single-centre academic cohort. Specific markers were evaluated for early and long-term mortality in patients with TIPS placement for refractory ascites or variceal bleeding.
METHODS
Data of electronic health records of patients who underwent a TIPS placement in the Amsterdam University Medical Center, location Academic Medical Centre (AMC) between October 2001 and November 2016 were collected in a database. All patients with cirrhosis over the age of 18 years who received a PTFE-covered TIPS were included. Patients who received a TIPS for non-cirrhotic portal hypertension were excluded.
The following data were collected: age, gender, aetiology of cirrhosis, indication for TIPS, date and cause of death, baseline laboratory tests prior to TIPS placement, follow-up data regarding complications, development of HE, treatment outcome, details regarding TIPS placement (stent-size, dilatation, pressure measurements), reinterventions, and radiological follow-up data. MELD score was calculated with the following formula and associated assumptions: (0.957 * ln(serum creatinine in mg/dl) + 0.378 * ln(serum bilirubin in mg/dl) + 1.120 * ln(INR) + 0.643) * 10” (https://www.mdcalc. com/meld-score-original-pre-2016-model-end-stage-liverdisease). If only a prothrombin (PT) value was available, internationalised normal ratio (INR) value was derived from the PT value using corresponding normal limits.
The electronic health record (EHR) was the primary data source. Missing clinical data were supplemented with data of paper patient files from the medical archive, data of referring hospitals EHRs, and information available at general practitioners. Missing radiological data were supplemented after reviewing the original images with an interventional radiologist (OvD).
Survival was defined as liver transplantation-free survival. Patients undergoing liver transplantation were censored at the day of transplantation. Patency of the TIPS was defined as last known Doppler US without signs of TIPS thrombosis or stenosis before liver transplantation, or previous re-interventions of a non-patent TIPS. To validate clinical improvement of ascites, this had to be either objectified by US or by physical examination, as documented in the EHR. New onset or deterioration of HE was interpreted from the EHR, using the West-Haven criteria. Rebleeding was defined as a documented variceal bleeding after TIPS placement. The study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as reflected in approval by the Medical Ethics Committee of the Academic Medical Centre in Amsterdam (reference number W17_093#17.112). For this type of study (retrospective) formal written consent was not required.
STATISTICS
Descriptive variables were expressed as mean (±SDs). Survival analyses were performed using Kaplan Meier curves, considering transplant-free survival. Log-rank test was used to compare cumulative survival among the groups. Independent t-test was used to compare numerical variables among groups, if normally distributed. Mann-Whitney U-test was used if numerical values were not normally distributed. Multivariate analysis was performed using Cox regression. All statistical analyses were performed with SPSS software (version 25.0; SPSS, Chicago, Illinois). Reported p-values are 2-tailed and considered statistically significant when the p-value was < 0.05.
Results
A total of 153 consecutive patients undergoing PTFE-covered TIPS placement were identified. Application of the exclusion criteria resulted in a total of 136 patients who were eligible for further exploration. Thirty-three patients were excluded from analysis since they were lost to follow-up. In total, 103 patients were included for analysis. A flowchart is provided in figure 1.
Baseline characteristics
Mean age at TIPS placement was 59 (± 12) years. Baseline characteristics are shown in table 1. Baseline characteristics for patients with variceal bleeding and refractory ascites are shown in
table 2. Aetiology of liver cirrhosis was distributed equally between the two groups. Patients who presented with variceal bleeding were younger, had lower platelet counts, and lower serum albumin levels, while patients with refractory ascites had higher serum creatinine levels and lower sodium levels. There was no difference in MELD scores between these two patient groups.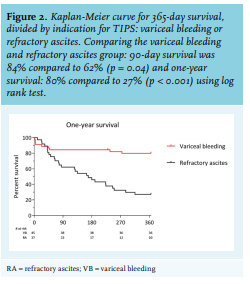
Transplantation-free survival
Four patients underwent liver transplantation within 90 days after TIPS placement. Another three patients after this period. Ten patients (10%) died within the first 30 days. One patient suffered from acute congestive heart failure and in six patients, liver and/or renal function deteriorated (all these patients had a MELD score of 20 or above at TIPS placement). These high MELD scores were mainly based on high bilirubin levels, implicating impaired liver function. Two other patients died of sepsis and one of a cerebral haemorrhage. Within the first 90 days, a total of 25 patients had died (24%). The overall one-year transplant-free (TF) survival rate in this cohort was 56%.
Figure 2 shows the transplant-free survival of the patients with refractory ascites and variceal bleeding. Ninety-day survival rate was 84% in the variceal bleeding group and 62% in the refractory ascites group (p = 0.04). Survival rates after one year were 80% for patients with variceal bleeding and 27% for patients with refractory ascites (p < 0.001).
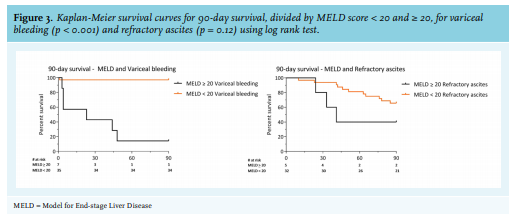
Cumulative survival at 90 days for patients with variceal bleeding and a MELD score < 20 was 97%, compared to 14% in patients with variceal bleeding and a MELD score ≥ 20 (p < 0.001; figure 3). Patients with refractory ascites had a 90-day survival of 66% when MELD score < 20, compared to 40% with MELD score ≥ 20 (p = 0.12).
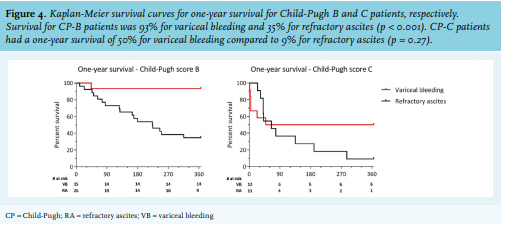
Kaplan-Meier survival curves, divided by Child-Pugh (CP) scores for variceal bleeding and refractory ascites are shown in figure 4. For patients with CP-B cirrhosis and variceal bleeding, one-year survival was 93% and 35% for CP-B patients with refractory ascites (p < 0.001). There was a trend for better one-year survival in patients with CP-C liver cirrhosis in patients with variceal bleeding (50%) compared to 9% in patients with refractory ascites.
Risk factors for mortality
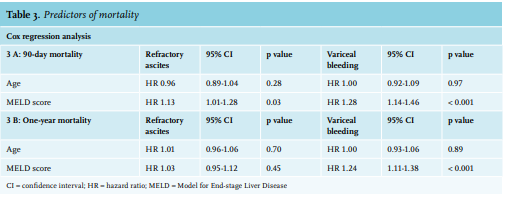
Risk factors for 90-day and one-year mortality, identified by Cox regression analysis, are shown in table 3. Factors were divided by the indications variceal bleeding and refractory ascites. For patients with variceal bleeding, as well as for patients with refractory ascites, a higher MELD score was a risk factor for 90-day mortality (HR 1.28 per MELD point increase, 95% CI: 1.14-1.46, p < 0.001 for variceal bleeding, and HR 1.13 per MELD point increase, 95% CI: 1.01-1.28, p = 0.03 for refractory ascites), while age was not (HR 1.00, 95% CI: 0.92-1.09, p = 0.97 for variceal bleeding, and HR 0.96, 95% CI: 0.89-1.04, p = 0.28 for refractory ascites). For one-year mortality, MELD score was only a risk factor for patients with variceal bleeding (HR 1.24, 95% CI: 1.11-1.38, p < 0.001) and not for patients with refractory ascites (HR 1.03, 95% CI: 0.95-1.12 p = 0.45).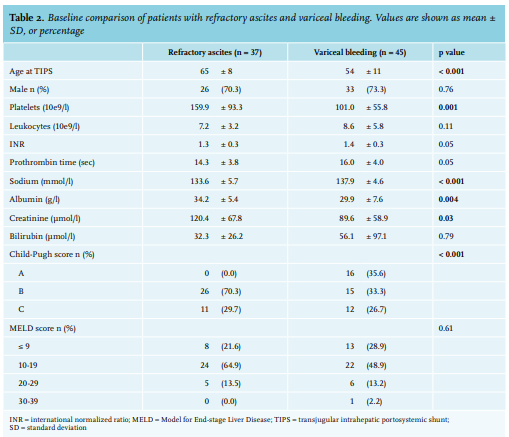
Outcome variceal bleeding
Rebleeding from oesophageal or gastric varices within 90 days occurred in 2 of 45 patients (4.4%), both CP-C and within the first two weeks. Overall rebleeding rate within 12 months was 8.9%: a success rate to control bleeding of 91%.
Outcome refractory ascites
Figure 5 shows the outcome for refractory ascites patients after TIPS placement. Within 90 days after TIPS placement, 14 patients died (38%). Of the remaining patients, 12 of 23 (48%) showed clinical improvement of ascites, while the other half did not improve clinically in this first follow-up period. After six months, 22 patients (49%) had died. A total of 12 patients clinically improved and 6 patients had no clinical improvement of ascites. After 12 months, 27 patients had died (73%). Of the remaining patients alive (n = 10), 80% had benefit of TIPS placement. Two patients did not show clinical improvement after 12 months. 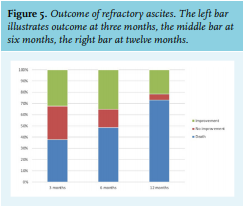
Development of HE after TIPS
Clinically manifest HE within 30 days was reported for 37 patients (36%). Closure of the TIPS was necessary in two patients to resolve HE; all others could be treated with either lactulose or lactulose in combination with rifaximin. Three patients (2%) developed a coma hepaticum, of whom two died and one recovered with administration of oral and rectal lactulose.
TIPS patency and re-interventions
After 90 days, re-intervention free survival was 86%. Cumulative percentages of re-intervention free survival declined to 80% after two years (Mean time to re-intervention: 88 days (+ 74), range 6-230 days, median 71 days) A total of 166 Doppler US examinations were included for further analysis. Six TIPS revisions were performed after abnormalities were found during follow-up on Doppler US examination (3.6%) (thrombosis, stenosis, or flow change). All patients had clinical symptoms, most often increased ascites. Revisions were performed in 13 patients who had clinical symptoms and inconclusive Doppler US studies (7.8%). A total of 147 routine Doppler US procedures (88.6%) did not reveal any indications for re-intervention.
DISCUSSION
In this retrospective study, a markedly better one-year transplant-free survival was found in patients who had a TIPS placement for variceal bleeding (80%) in comparison to refractory ascites (27%) (p < 0.001). Survival was poor in patients with a MELD score ≥ 20, both in patients with variceal bleeding and refractory ascites. The number of reinterventions, after abnormalities on Doppler US were found, were low compared to the total number of performed surveillance Doppler US. Therefore, the need for ultrasound surveillance after TIPS placement can be questioned and probably does not add significant information to clinical evaluation.8 We suggest that Doppler US can be left out of the follow-up in patients with ascites, since almost all patients had a clinical increase in ascites as a result of TIPS dysfunction. For patients with variceal bleeding this might still be a point of debate, since a rebleed could be associated with a higher mortality.9
Patients with CP-B and variceal bleeding had a better one-year survival (93%) compared to CP-B patients with refractory ascites (35%) (p < 0.001). On the other hand, in the first 30 days after TIPS placement, CP-C patients with variceal bleeding had a worse prognosis compared to patients with refractory ascites. This was probably due to the advanced disease state as variceal bleeding is a known life-threatening complication with high mortality in CP-C patients within the first days.9
After more than 30 days, prognosis was better for patients with variceal bleeding. After TIPS, the control rate of bleeding is high, and once bleeding is controlled in a patient, survival is relatively stable. Moreover, patients with refractory ascites often have more advanced liver disease, reflected by more patients with CP-B and CP-C cirrhosis in this group. Besides, patients with refractory ascites were also older in our cohort.
This study population showed an incidence of post-TIPS HE of 36%, which is in agreement with previously reported studies (15-54%).4,5 However, this might be an underestimation due to the retrospective nature of this study and missing information to complete the West-Haven criteria. Treatment of post-TIPS HE is dependent on the severity and is patient specific. Mainly lactulose enemas were used in more severe cases whereas oral lactulose was the preferred first-line treatment in stage I-II HE. In two occasions, the TIPS had to be occluded to reduce complaints of HE. Post-TIPS HE is a severe complication, and unfortunately not easy to predict. Therefore, more studies in larger groups are needed to find markers that could select high-risk patients. Currently no prophylactic treatments are available to prevent post-TIPS HE. However, recently a multicentre, randomised, placebocontrolled, double blind study has started (NCT 04073290) to assess the prophylactic administration of rifaximin and lactulose to prevent post-TIPS HE.
The overall incidence of post-TIPS HE declined over time in our study cohort. One could suggest that this was the result of the introduction of rifaximin in the Netherlands in 2010. However, rifaximin is only prescribed to patients to prevent a third episode of clinical manifest HE while a history of clinical manifest HE is a contraindication for TIPS placement. We therefore presume that better and stricter selection of patients in combination with an increasing experience within our hospital with the use of TIPS in patients seems to be a more plausible explanation for the decline of HE over time.
Approximately 50% of patients with refractory ascites who survived 90 days after TIPS placement reported clinical improvement. This increased to 68% after 6 months, and 80% after 12 months. Although one-year survival of patients with refractory ascites was only 27%, response rates were aligned with current literature (35-85%).6,10 Therefore, in selected patients with refractory ascites, TIPS could be valuable. Standard post-TIPS diuretics dosage was 50% of the pre-TIPS dosage; further reduction was based on the clinical signs of the patient.
Control of variceal bleeding within the first year in our population was reached in 91% of the patients. This is similar to percentages mentioned in literature.6 Early rebleed occurred in 4% of the patients and was lower compared to the 12.4% reported earlier.6 However, uncovered stents were used in this previous study whereas only PTFE-covered stents were used in our cohort. It is unlikely that rebleeds were missed due to presentation elsewhere, because rebleeds are highly correlated with TIPS patency, which was reported back to our hospital. TIPS patency was examined in a standardised manor with Doppler US. Flow velocities were compared to previous known velocities and flow direction was assessed. Patients who were evaluated for possible TIPS dysfunction all suffered from increased amount of ascites and clinical deterioration. Therefore, we suggest that routine follow-up should be implemented differently in the future. Follow-up by Doppler US can be omitted in patients with refractory ascites, if those patients do not suffer from (increased) complaints after TIPS placement. Patients, in whom the indication for TIPS was variceal bleeding, can be monitored less strictly than the current protocol, since TIPS patency rates are very high. Patients with cirrhosis are screened every six months for hepatocellular carcinoma at the outpatient clinic, and TIPS flow can be measured during this surveillance US if necessary. Our data support previous recommendations that regular surveillance is not necessary in the era of PTFE-covered stents.11-14 A Doppler US examination might well be used to validate initial patency and to measure initial flow velocities. For further follow-up, Doppler US examination should only be done on indication.8 Our study has limitations. The retrospective nature of this study in combination with the relatively small number of patients in each group and missing data of incomplete patient records might have caused underreporting. Outcome values were reported as part of daily clinical practice and were not part of a study protocol, so could be biased by the reporting physician. Therefore, besides survival data, outcomes were not always exactly measured at the time points of 3, 6, and 12 months. The surprisingly high level of serum albumin in the refractory ascites group is difficult to explain and could be artificially high due to pre-procedural albumin suppletion.
In conclusion, overall transplant-free survival in our cohort was lower than previously reported mainly due to low one-year survival in patients with refractory ascites. Patients with variceal bleeding had an excellent overall one-year survival and very effective control of variceal bleeding. Routine Doppler US surveillance after PTFE-covered TIPS placement appears unnecessary as TIPS dysfunction was indicated by clinical deterioration rather than abnormalities found on routine Doppler US examinations.
ACKNOWLEDGEMENTS
No funding or financial support was received for the conduct of this study or preparation of this manuscript. The authors declare that they have no conflicts of interest related to this manuscript.
We kindly thank
Dr. L.C. Baak (Onze Lieve Vrouwe Gasthuis Oost, Amsterdam), Dr. J. Blokzijl (UMC Groningen, Groningen), Drs. A.C.T.M. Depla (MC Slotervaart, Amsterdam), Dr. P.W. Friederich (Meander Medisch Centrum, Amersfoort), Drs. E.J. van Soest (Spaarne Gasthuis, Hoofddorp), Dr. P.C.F. Stokkers (Onze Lieve Vrouwe Gasthuis West, Amsterdam), and Dr. X.G. Vos (Westfriesgasthuis, Hoorn) for their cooperation during collection of follow-up data.
REFERENCES