KEYWORDS
Computational fluid dynamics, fibromuscular dysplasia, functional measurements, renal artery stenosis, renovascular disease, secondary hypertension
INTRODUCTION
Renal artery stenosis is, in most cases, a result of atherosclerosis. In ~ 10% it is caused by fibromuscular dysplasia (FMD), a connective tissue disorder of unknown origin with a predilection for the renal arteries.1 Renal artery stenosis is a well-established cause of secondary hypertension, but the success of percutaneous interventions on blood pressure, although generally better in patients with FMD,2 is variable. Second, atherosclerotic renal artery stenosis (ARAS) is associated with an increased risk of renal failure and mortality.3,4 In the Netherlands, renovascular disease was the primary cause of renal replacement therapy in 11% of patients in 2017.5 Treatment of renal artery stenosis, however, has declined sharply in the past few years following the publication of randomised trials that showed that angioplasty with stent placement of the renal arteries over and above medical treatment was not better compared to conventional (medical) treatment alone.6-8 This strong decline in percutaneous interventions is somewhat surprising as the trials explored indications where the benefit of intervention was uncertain and excluded patients with uncontrolled or treatment resistant hypertension, recurrent flash pulmonary oedema, or refractory heart failure. Although past trials showing advantages of stent placement in patients with resistant hypertension and acute pulmonary oedema had limitations in design and sample size,9-12 recent (non-randomised) experiences continue to suggest that stent placement is beneficial if existing selection criteria are applied.13,14 While in ARAS blood pressure can significantly improve after stent placement, percutaneous renal intervention in patients with FMD has been reported to completely cure hypertension in 36% of cases.15 In older patients, a conventional approach for FMD can also be considered, as the chance of curing hypertension after an intervention diminishes significantly with age.15 In other words, for both ARAS and FMD, better diagnostic strategies are necessary to identify patients who are most likely to benefit from revascularisation. In the present overview, we provide a summary of ongoing initiatives to improve the diagnosis and treatment of patients with renal artery stenosis. 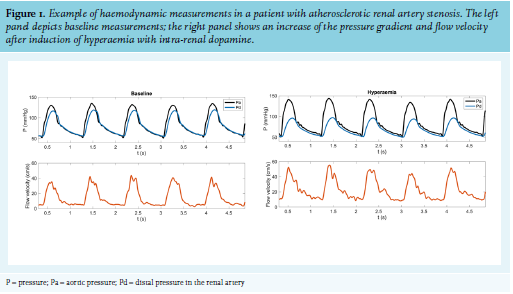
New diagnostic possibilities for renal artery stenosis
Animal experiments have shown that acute renal artery stenosis must be above ~60% diameter loss to alter the pressure gradient and above 75% to cause a reduction in renal blood flow,16 although these cut-off values are known to depend on stenosis eccentricity. Clinical evidence regarding the anatomical degree above which percutaneous interventions would be useful is limited. This may either result from difficulties related to the accuracy of anatomical grading, the paucity of data in patients with severe anatomical lesions (often excluded from randomised trials), and residual kidney function. Efforts to improve patient selection by ultrasound, renal scintigraphy, and renal vein sampling have, in general, been unsuccessful,17,18 and combining anatomical grading with the measurement of translesional pressure gradients have, so far, yielded mixed results.19,20 New developments that combine pressure and flow measurements, on the other hand, have yielded promising results in patients with coronary artery disease and may be useful in patients with renal artery stenosis. In parallel to these invasive measurements, advances in imaging techniques and computer modelling have generated the possibility to determine the functional consequences of renal artery stenosis using computational fluid dynamics (CFD).
Fractional flow reserve and renal flow reserve
Studies performed in the coronary circulation have shown that anatomical abnormalities have a limited association with functional significance.21,22 Assessment of functional characteristics by pressure gradient measurements using sensor-equipped wires under hyperaemic conditions is recommended in current guidelines as it is superior over angiography-guided revascularisation, and has significantly improved clinical outcomes in patients with coronary artery disease.23-26 In addition to pressure measurements, direct measurement of coronary flow velocity under baseline and hyperaemia can assess microcirculatory status, which has prognostic value in patients with and without significant coronary artery stenosis.27-29
Using similar techniques, it is possible to reproducibly measure pressure and flow velocity under baseline and hyperaemic conditions in the renal artery.30 In the renal circulation, maximal hyperaemia can be achieved by an intrarenal bolus of dopamine 30 μg/kg.30 ,31 As depicted in figure 1, the renal fractional flow reserve is derived from the pressure measurements, which quantify the haemodynamic significance of the stenosis.
From the flow measurements, the renal flow reserve is determined, which expresses to which extent the microcirculation can increase flow relative to resting conditions. As the stenosis gradient is dependent on the achieved hyperaemia and the maximal flow rate is related to the pressure loss over the stenosis, these measurements are interdependent. This suggests that, similar to the coronary circulation, the combined pressure-flow measurements can be used to distinguish primary macrovascular from predominant microvascular disease, which may aid in patient selection for renal revascularisation therapy (figure 2). Earlier studies have shown promising results using only hyperaemic pressure measurements, but it has been difficult to validate specific cut-offs.32 In the recently started Functional Renal Haemodynamics in Patients with Renal Artery Stenosis study (HERA-3, Netherlands Trial Registery NL8408), the predictive ability of combined pressure and flow measurements for treatment success will be investigated using ambulatory blood pressure and iothalamate/hippuran renal function measurements as outcome. HERA-3 will also investigate the validity of non-invasive flow simulation techniques to estimate the translesional pressure gradient.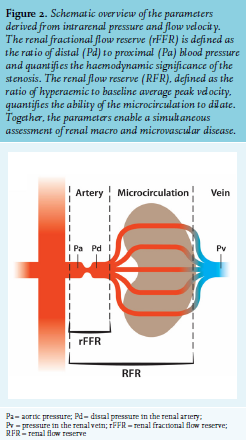
Computational fluid dynamics
Computational fluid dynamics (CFD) uses numerical analysis and data structures to analyse and solve problems that involve fluid flows. With CFD techniques, the translesional pressure gradient for stenotic lesions and other hemodynamic metrics can be calculated based mainly on an anatomic model of a patient’s arteries. In this three-dimensional anatomical model, CFD solves the physical equations that govern the motion of blood. The computed solution includes details on the acceleration of blood through the stenosis, as well as the disturbed motion of blood downstream of the stenosis and the pressure loss associated with these disturbances. Over the past decade, CFD has seen an increasing adoption for biomedical research. More recently, CFD software has been commercially developed33 and validated34 for an improved clinical classification of coronary artery disease. This has been made possible by advances in medical imaging, segmentation techniques, and computational power, all of which are likely to experience further improvements in the coming decade.
A CFD simulation of renal artery stenosis can non-invasively derive the translesional pressure gradient under various levels of renal blood flow. For this CFD simulation, two primary inputs from patient data are needed to accurately inform the model. The first is a three-dimensional geometry of the stenosis, including the juxtarenal aorta. This geometry can be segmented from high-resolution contrast-enhanced CT or MRI scans, preferably with a slice thickness below 1 mm. Second, the renal blood flow rate through the stenosis must be directly or indirectly specified for the simulation. A strength of the CFD model is that both a resting flow rate, as well as a high flow rate mimicking hyperaemia can be simulated. The difference in translesional pressure gradient of a haemodynamically significant stenosis relative to a non-significant stenosis will be amplified at higher flow rates, as the gradient scales quadratically with flow.35 Therefore, the translesional pressure gradient during maximal flow appears to be a better predictor of treatment success than measurements in the resting state.32
For the HERA-3 study, a CFD model will be simulated for all individual patients, and the modelled resting and hyperaemic pressure drop will be compared to the invasive measurements. An example of a CFD simulation of a patient with a moderate RAS is shown in figure 3, which was performed with the open-source SimVascular software (release 23-05-2018, http://simvascular.github.io/).36 The CFD simulation for this patient predicted a hyperaemic pressure drop of 34 mmHg, compared to an invasively measured gradient of 38 mmHg (with an aortic pressure of 160 mmHg, this corresponds to a renal fractional flow reserve of 0.45 and 0.43 for the CFD simulation and measurement, respectively). After per-patient measurement and simulation, the accuracy of the CFD simulation will be assessed and its predictive value for blood pressure response to treatment will be investigated. If sufficiently predictive, the non-invasive CFD simulations can become a valuable tool in the diagnostic workup in patients with ARAS or FMD, although the anatomical characteristics of FMD may prove more challenging for the CFD technique.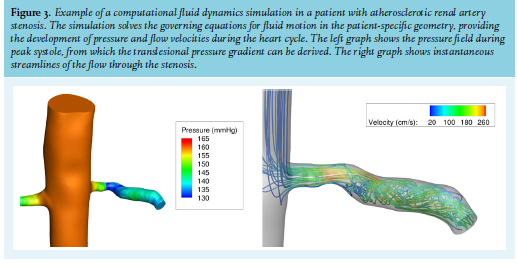
Imaging in FMD
The diagnosis of FMD is based on imaging studies with typical non-atherosclerotic vascular lesions (by definition in the absence of syndromal or inflammatory diseases).2,37 FMD is classified into two subtypes by its angiographic presentation: multifocal FMD with a typical string-of-beads appearance and unifocal FMD with one or more focal or tubular stenoses. Distinguishing unifocal FMD from ARAS is often difficult, and therefore, the diagnosis is limited to younger patients (< 40 years) without risk factors for atherosclerosis and without arterial calcifications on imaging studies. In general, patients with unifocal FMD are younger and have more severe hypertension.38 Moreover, the effect of unifocal FMD on functional parameters of the kidney resembles that of ARAS, with reduced kidney perfusion and an increase in renin secretion.39 In multifocal FMD, however, kidney perfusion and microvascular function are more or less intact, and renin secretion is comparable to patients with essential hypertension.40 Therefore, these two FMD subtypes are generally considered to be different disease entities. The gold standard for the diagnosis of FMD is digital subtraction angiography (DSA).2 Both renal arteries should be selectively catheterised, as FMD lesions are predominantly located in the middle or distal renal artery which can be overlooked with aortic angiography alone. To obtain a more detailed view, optical coherence tomography or intravascular ultrasound can be used.41,42 Duplex ultrasound is generally not recommended as its negative predictive value is low and the exam is highly operator-dependent.2,43 Over the past years, the resolution of computed tomography angiography (CTA) has improved considerably, which has increased the use of CTA as an alternative to DSA. As CTA is non-invasive, cheaper, and allows imaging of several vascular beds in one scan; it is currently recommended as the first diagnostic step in case of clinical suspicion for FMD. CTA is preferred over magnetic resonance angiography (MRA) as its spatial resolution is higher. However, as the spatial resolution of CTA is inferior to DSA, smaller lesions could still be missed on CTA. This is illustrated by two prospective studies in whom all patients underwent DSA, regardless of the results of previous MRA or CTA. Although these studies used older MR and CT scanners (slice thickness of 2.5-3 mm) than the ones currently used, sensitivity for FMD was only 28% for CTA and 22% for MRA (as compared to DSA) in one study.44 Presumably, sensitivity has been improved with the newer generations of CT and MR scanners (slice thickness ~0.6 mm), but its value has not been evaluated yet. Moreover, we are aware of several cases with (false) negative CTA or MRA imaging, in whom FMD lesions were found with DSA. Therefore, in case of high clinical suspicion of FMD, DSA should be considered even if CTA or MRA imaging are negative.
Treatment of FMD
In patients with hypertension due to renal FMD, treatment with balloon angioplasty appears to be safe and effective in lowering blood pressure. Balloon angioplasty can cure hypertension (BP < 140/90 without antihypertensive medication) in ~36% of patients with FMD,15 and in those patients not fully cured, improvement in renal function,45,46 blood pressure,47-49 and reduced use of antihypertensive drugs50,51 has been reported. However, these data were derived from observational studies, as randomised controlled trials on revascularisation in FMD are lacking. Nevertheless, balloon angioplasty is more effective in lowering blood pressure in patients with FMD than in ARAS. Presumably, this difference in response to revascularisation is caused by atherosclerotic damage to the intrarenal microvasculature in kidneys with ARAS, while microvascular function is more or less intact in kidneys with FMD.52,53 Surgical revascularisation in FMD is usually reserved for patients with complex lesions or after failure of balloon angioplasty, as balloon angioplasty is less invasive with a lower risk for major complications (15% with surgery versus 6% with balloon angioplasty).15 Stent placement is discouraged in FMD as several cases of stent fractures have been reported. Presumably, this is caused by the fact that multifocal FMD lesions are typically located in the middle or distal two-thirds of the renal artery (in contrast to ARAS or unifocal FMD), where the amplitude of movement due to respiration or exercise is higher. However, not placing a stent increases the risk of restenosis, which occurs in 10-38% of patients (depending upon duration of follow up).15,51,54 Hence, for patients whose blood pressure rises over time, a second balloon angioplasty should be considered. Because observational studies suggest that the efficacy of balloon angioplasty decreases with age, duration of hypertension, and the presence of kidney damage,15,55 balloon angioplasty should particularly be considered in young patients or in patients with recent onset hypertension. In elderly patients without severe hypertension or hypertension that responds well to antihypertensive drugs, conservative management is often preferred and reasonably effective.56,57 As not all patients with renal artery FMD develop hypertension, it is conceivable that the FMD lesions are an innocent bystander in a substantial proportion of hypertensive patients. Future randomised controlled trials are needed to assess the true effect of balloon angioplasty in FMD. Aforementioned techniques such as fractional flow reserve and renal flow reserve measured with a thin pressure wire, as well as computational fluid dynamics, could prove useful for predicting treatment response.
The Dutch Fibromuscular Network
Following a 2014 publication of the European Consensus Statement on the diagnosis and management of FMD,2 a European Registry was set up to gather information on FMD patients across Europe.43 By the end of 2019, this initiative has included over 1000 patients, of which the first results of the analyses are expected in 2020. There has been a substantial contribution from centres in the Netherlands and this has prompted Dutch investigators to start working together and to form their own national network, The Dutch Fibromuscular Network. So far, the Network consists of vascular medicine specialists in Maastricht, Utrecht, Amsterdam, Rotterdam, Nijmegen, Sittard, and Tilburg. In close collaboration with the radiologists in their hospitals, these specialists have drawn up a general protocol for the evaluation of patients who are suspected of having FMD. This protocol includes mandatory data on the history, physical examination, and laboratory values, as well as the type and extent of imaging. The uniformity in patient approach will thus allow the establishment of a Dutch FMD Registry. Other centres wishing to participate in the Network are welcome to do so as long as they adhere to the common protocol. The Network is actively supported by patients with FMD (www.fmdgroep.nl).
CONCLUSION
Renal artery stenosis is a common cause of secondary hypertension. Renal revascularisation can potentially cure or significantly improve blood pressure control, but the response to revascularisation is hard to predict. Therefore, new diagnostic strategies are needed for optimal patient selection. Research initiatives, including the Dutch Fibromuscular Dysplasia Network, aim to elucidate the aetiology of FMD and improve its identification and management.
ACKNOWLEDGEMENTS
The HERA3 study is supported by an innovation grant (project number 19OI18) from the Dutch Kidney Foundation.
DISCLOSURE
All authors declare no conflicts of interest. LvdV, LV, and BJvdB received an innovation grant from the Dutch Kidney Foundation for the HERA3 study (DKF project code 19OI18).
REFERENCES