KEYWORDS
Colonoscopy, endoscopy, gastroscopy, iron deficiency anaemia, salicylate
INTRODUCTION
When there is no overt bleeding source, iron deficiency anaemia (IDA) is most frequently due to occult gastrointestinal blood loss. An evaluation of the gastrointestinal tract by gastroscopy and/or colonoscopy is therefore the standard in diagnosing the cause of IDA.1-3 A gastrointestinal lesion explanatory for IDA is found in about two-thirds of the patients who are evaluated with gastroscopy or colonoscopy.1,4-8 Known positive predictive factors for finding explanatory pathology in endoscopy are higher age, male gender, a low mean corpuscular volume, and a positive faecal occult blood test (FOBT).9-11
Salicylates are widely used in low doses to prevent cardiovascular and cerebrovascular disease.12 Because it is known that salicylates can cause erosions and spontaneous micro-bleeding of the gastrointestinal mucosa,13-15 it can be hypothesised that salicylates could cause iron deficiency anaemia, even in the absence of visible abnormalities upon gastrointestinal endoscopy. This would make the use of salicylates a negative predictive factor associated with finding explanatory pathology for IDA during an endoscopy. On the other hand, we could assume that salicylates cause pathology like polyps, ulcers, and carcinomas to bleed more quickly, and that the use of salicylates would reveal this pathology earlier, making it a positive predictive factor for explanatory pathology findings. Literature about whether the use of salicylates is a positive or negative predictive factor for explanatory pathology findings for an IDA during gastroscopy or colonoscopy procedures is scarce and contradictory. Previous studies have concluded that salicylates can cause a small increase of occult gastrointestinal blood loss, although this was clinically irrelevant.16,17 Some studies found no relation between the use of salicylates and explanatory pathology findings.8,9 However, in a group of elderly patients with IDA, it was observed that significantly less explanatory pathology was identified in patients who were using salicylates.18 The review of Banerjee et al. states that in patients who use anticoagulants in general, colon polyps and carcinomas can be revealed earlier compared to patients who are not using anticoagulants.19
Knowledge of the impact of salicylate use in determining a clinically-relevant disease in patients with IDA is important as it might influence the pre-test probability of detecting explanatory pathology with a gastrointestinal endoscopy. This is especially important because the procedure is invasive and often performed in elderly and fragile patients. Knowing the pre-test probability of finding explanatory pathology can help physicians with decision making regarding whether to perform a gastrointestinal endoscopy in these groups of patients.
The aim of this study was to determine whether the use of salicylates is a predictive factor for finding explanatory pathology in gastroscopy or colonoscopy in patients with IDA.
MATERIALS AND METHODS
Study population
The study population consisted of patients who underwent a gastroscopy and/or colonoscopy to determine the cause of IDA at Treant Healthcare, hospital location Scheper in Emmen, the Netherlands. A record search was done in the hospital information system to find all patients who were diagnosed with an IDA in the period between January 1st, 2011 and December 31st, 2016. Because an IDA diagnosis was probably changed to a new diagnosis in the hospital information system if a cause was found, a search was also performed for the diagnoses that could be explanatory for IDA. Of this last group, only the patients who underwent a gastroscopy and/or colonoscopy because of an IDA were included. An IDA was defined as a haemoglobin concentration below 8.5 mmol/l for men and below 7.5 mmol/l for women, in combination with a ferritin level below 30 µg/l.20 In patients with a clear acute process, the ferritin level could not be used because ferritin is also an acute phase reactant.21 In these cases, a diagnosis was also considered an IDA if, in addition to a low haemoglobin concentration, the mean corpuscular volume was below 80 fl, the transferrin level was above 45 µmol/l, or the serum iron was below 14 µmol/l.
The study compared two groups. The first consisted of patients who were not using antithrombotics at the time of, and six months prior to, the gastroscopy or colonoscopy. The second group consisted of patients who used a salicylate at the time of, and at least during the last six months prior to, the gastroscopy or colonoscopy. Patients were not excluded if their salicylate was temporarily stopped for seven days to reduce the bleeding risk during endoscopy. Patients who used antithrombotics other than a salicylate were excluded. Because of the changed a priori chance, patients were excluded if, prior to the endoscopy, a radiological evaluation or a FOBT was performed. Patients who underwent only one of the endoscopies, either a gastroscopy or a colonoscopy, were included if the reason for not continuing the other endoscopy was the finding of relevant pathology during the first endoscopy. If visibility during endoscopy was poor, due to unsuccessful bowel cleansing or for other reasons, patients were excluded, unless a second successful endoscopy was performed. Most patients underwent biopsies to diagnose coeliac disease. Exceptions were made if the a priori chance of coeliac disease was very low, for example in elderly patients. The decision whether to perform biopsies was individualized and was made by the attending physician. The outcomes of other diagnostic tests performed after the endoscopic evaluation were not included in this study. Because of the increased chance of anaemia, patients with haematological diseases were excluded. Patients with gastrointestinal tract malignancy in their medical history were excluded because of the increased a priori chance for a recurring malignancy and because of the possibility of earlier proceeding to perform an endoscopy in this group of patients, for example to reassure them.
All data of included patients were stored anonymously in a database: gender, age at the time of the endoscopy, the use of salicylates, whether an explanation for the anaemia was found during gastroscopy or colonoscopy, and whether a complication of the gastroscopy or colonoscopy had occurred. The following diagnoses were considered explanatory for an IDA: colorectal malignancy, colon polyps ≥ 1 cm,19,22 inflammatory bowel disease, angiodysplastic lesions, reflux oesophagitis with erosions that were at least 5 mm long (stage B, C, or D), erosive gastritis, coeliac disease, oesophageal cancer, gastric cancer, small bowel cancer, and peptic ulcers. Like in other studies, diverticula of the colon were not considered explanatory for an IDA.1,3,4,5,8
The primary research parameter was in how many cases an explanatory diagnosis was found for IDA during gastroscopy or colonoscopy, and if there was a difference between the two groups. Furthermore, the number of complications was compared between the two groups.
Statistical analyses
A power analysis was conducted with a set at 5% and β at 20%. Based on literature, it was expected that in about two-thirds of the cases an explanatory diagnosis would be found. A difference of 25% between the two groups was considered clinically relevant. The number of patients required was 137 per group.
The statistical analyses were conducted with the program IBM SPSS Statistics version 22. Since age was not normally distributed, a Mann-Whitney test was performed to study the difference in age between the two groups. Dichotomous data (salicylate use, explanatory finding, complications) were compared with the Fisher’s exact test. To analyse whether an association existed between independent variables (salicylate use, age, gender) and the outcome variable (explanatory finding), univariate logistic regression analyses were used. To correct for confounders, a multivariate logistic regression analysis was performed. A p-value ≤ 0.05 was considered statistically significant. A receiver operating characteristic curve (ROC curve) was created to determine the diagnostic value of the model used in multivariate logistic regression analysis, and the area under the curve (AUC) was determined. The diagnostic value was considered significant if the 95% confidence interval of the AUC was above 0.5.23
RESULTS
In total, 464 patients were included, 174 who used a salicylate and 290 who were not using a salicylate. Table 1 shows the patient characteristics of the total sample and of the separate groups. Median age was significantly higher in the group of salicylate users than in the group of patients who were not using a salicylate (p < 0.001). Also, gender was significantly different between the two groups (p = 0.004), with significantly more male patients in the group of salicylate users. Explanatory pathology for IDA was found in 41.2% of the patients, which was not significantly different between the group of salicylate users and the group that did not use salicylate. Table 2 shows the identified pathology and frequency per group. A complication occurred in only two of the 464 patients: a perforation after colonoscopy in a patient who used a salicylate and a bleeding after colonoscopy in a patient who did not use a salicylate.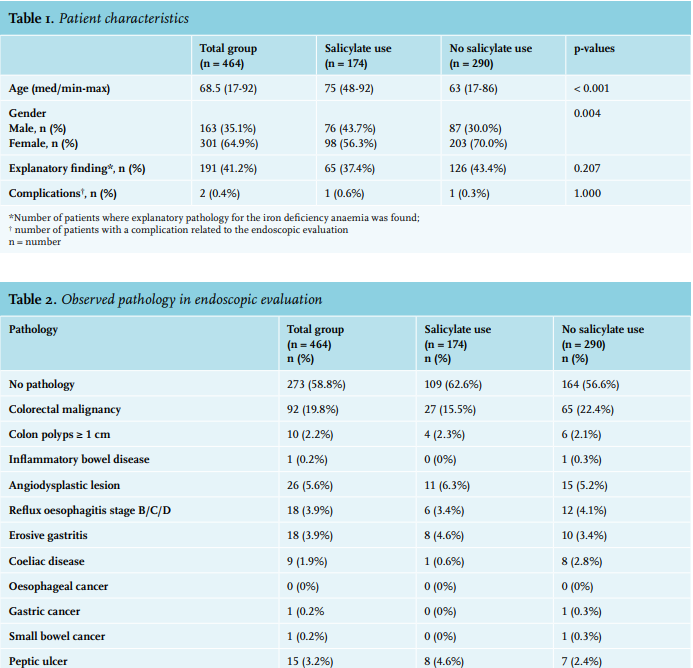
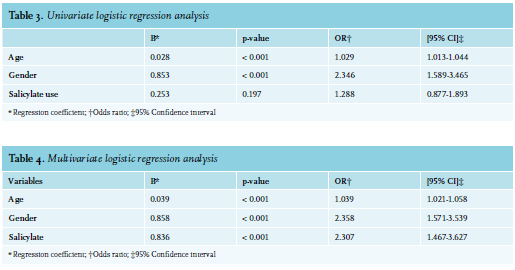
Univariate logistic regression analysis showed that both age and gender were significantly related to finding explanatory pathology at gastroscopy or colonoscopy (table 3). The higher the age of the patient, the higher the chance of finding explanatory pathology, with an odds ratio of 1.029 per year difference in age (p < 0.001). Explanatory pathology was significantly more often found in males than in females, with an odds ratio of 2.346 (p < 0.001). In univariate analysis, the use of a salicylate was not a significant predictor for finding explanatory pathology.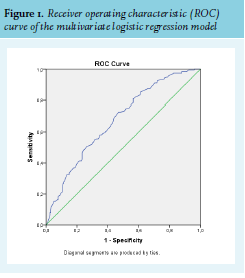
Since higher age and male gender were predictors for finding explanatory pathology, and since age was significantly higher in the group of salicylate users, which consisted of significantly more male patients, the variables age and gender were identified as possible confounders. A multivariate logistic regression analysis was therefore conducted (table 4), which showed that all variables were significantly related to finding explanatory pathology at gastroscopy or colonoscopy (all p < 0.001). After correction for age and gender, the use of a salicylate is, therefore, a negative predictor for finding explanatory pathology for IDA. Explanatory pathology is significantly more often found in patients who are not using a salicylate than in patients who are using a salicylate, with an odds ratio of 2.307. The area under the curve in the ROC curve was 0.673 (95% CI 0.624-0.722) (figure 1), indicating that the model has a significant diagnostic value.
DISCUSSION
Occult gastrointestinal blood loss is the most common cause of iron deficiency anaemia when there is no overt bleeding source.1-3 It is known that salicylates can cause erosions of the intestinal mucosa and an increase in gastrointestinal blood loss.13-15 This study showed that significantly less explanatory pathology for IDA is found during gastroscopy or colonoscopy in patients with IDA who are using salicylates.
At first, it appeared that no differences existed in the frequency of finding explanatory pathology between the group of patients who were using and the group of patients who were not using a salicylate. However, the salicylate users were significantly older and more often male. Higher age and male gender are known positive predictive factors for finding explanatory pathology in endoscopic evaluation in IDA.9-11 If salicylate use had no influence on finding explanatory pathology, it was expected that more explanatory pathology would have been found in the group of salicylate users. When correcting for age and gender, multivariate logistic regression analysis showed that the use of salicylates is a negative predictive factor for finding explanatory pathology. In previous studies, no relation between salicylate use and finding explanatory pathology was found.8,9 The reason for this might be, that in these studies, no corrections were made for age or gender differences in salicylate users and non-users. The outcome of our study not only supports previous findings in elderly patients with IDA, where a relation between salicylate use and a negative endoscopy was found, but also shows that the relationship between the use of salicylates and negative endoscopies is independent of age.18 Although previous studies stated that an increase in occult gastrointestinal blood loss was not significantly influenced by the use of salicylates, this study suggests the opposite because of more negative endoscopies in salicylate users.16,17
A limitation of this study is that the question whether salicylates can cause IDA cannot be answered, because the small intestine, where other explanatory pathology could have been located, was not evaluated with capsule endoscopy. Because the study was retrospective, it is also possible that no corrections were made for variables that could have influenced the probability of finding explanatory pathology, like the exact haemoglobin value or the mean corpuscular volume. In addition, the use of other medication was not taken into account.
Other studies showed that in about two-thirds of the patients, an explanatory finding for IDA is found during gastroscopy or colonoscopy.1,4-8 In this study, explanatory pathology was found in only 41.2% of the patients. A possible explanation is that, unlike those studies, patients were excluded from our study if a FOBT or radiological evaluation was performed prior to the endoscopic evaluation. It is likely that we may have thus excluded patients in whom explanatory pathology was more likely to be found, since a positive FOBT is a positive predictive factor for finding explanatory pathology, and radiological evaluation also influences the a priori chance for finding explanatory pathology. Another explanation could be that patients with a malignancy of the gastrointestinal tract in their medical history were excluded. It is likely that more explanatory pathology would have been found in this group of patients, due to the increased a priori chance of malignancy.
In conclusion, the use of salicylates should be considered as a negative predictive factor when predicting the outcome of an endoscopic evaluation in patients with IDA. Explanatory pathology for IDA is found significantly less often in patients who are using a salicylate than in patients who are not using a salicylate. Endoscopic evaluation will still be the standard for detecting relevant pathology, also in patients using salicylates. When there is doubt about performing an endoscopic evaluation, for example, in elderly and fragile patients, the use of salicylates should be included in the decision making of whether or not to perform an endoscopic evaluation in patients with IDA.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES