KEYWORDS
Cryoglobulinaemia, paraproteinemia, vasculitis, Waldenström’s macroglobulinaemia
INTRODUCTION
Vasculitis has a varied and nonspecific clinical presentation and extensive differential diagnosis.1,2 In this case report, we describe the diagnostic process from suspected vasculitis to established small vessel vasculitis based on monoclonal cryoglobulinaemia due to an underlying haematological disease. This case shows an uncommon cause of vasculitis and highlights that even a limited quantity of paraproteins can cause severe morbidity.
CASE REPORT
A 78-year-old man was admitted to our hospital with malaise, night sweats, and weight loss. Six months before, he was evaluated by a neurologist because of axonal polyneuropathy. Work-up revealed an IgM-kappa paraproteinaemia of < 1 g/l. He did not suffer from B symptoms at that time and there were no signs of lymphadenopathy or bone marrow invasion. IgM antibodies against myelin-associated glycoprotein were not detected. His further medical history reported a coronary artery bypass graft and treated tuberculosis in childhood. For the last two weeks, he reported malaise, night sweats, and weight loss. He felt progressive pain and stiffness in his legs during exercise, which was different from the previous neuropathic pain. Furthermore, he noticed a right-sided foot drop.
On physical examination there was no lymphadenopathy and examination of heart, lungs, and abdomen was unremarkable. We noticed livedo reticularis on both legs and bilateral pitting oedema. There were no signs of acrocyanosis or purpura. Peripheral pulsations were intact. Neurologic examination showed a paresis of the dorsiflexors of the right foot, suggestive for peroneus nerve damage. Initial laboratory tests showed mild normocytic anaemia, mild elevated C-reactive protein, and elevated creatinine kinase with normal liver and kidney function. 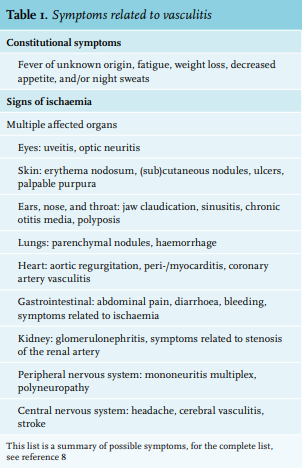
Because of the constitutional symptoms, livedo reticularis, and suspected myositis and mononeuritis multiplex, we considered a small vessel vasculitis (table 1).
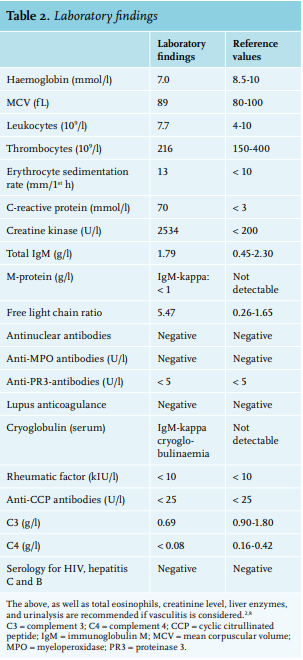
In order to identify the type of vasculitis and to consider the differential diagnosis of a malignancy or infection, additional laboratory tests (table 2) and a positron emission tomography/ computed tomography (PET-CT) scan followed.3,4 The PET-CT scan showed elevated uptake in the right upper leg and an additional magnetic resonance imaging (MRI) scan was suggestive for inflammatory myopathy of the vastus lateralis muscle. Biopsy of skin, muscle, and fascia from the right quadricep muscle showed perivascular infiltrates of predominantly lymphocytes with destruction of the small vessel walls. Together with fibrinoid degeneration, signs of leucocytoclasia, and thrombosis of the lumen, a leucocytoclastic vasculitis was diagnosed. Additional laboratory tests showed no evidence for an auto-immune aetiology or systemic rheumatic disease. Cryoglobulinaemic vasculitis was diagnosed due to the presence of cryoglobulins, which could be typed as type I (monoclonal IgM kappa). Bone marrow biopsy revealed slight infiltration of small B-cell non-Hodgkin lymphoma with plasmacytoid differentiation.Once the diagnosis of symptomatic Waldenström’s macroglobulinaemia was confirmed, we started first-line therapy:5-7 six courses of dexamethasone, rituximab (an anti-CD20 monoclonal antibody), and cyclophosphamide (chemotherapy). After six treatment courses, paraproteins and cryoglobulins were not detectable anymore and creatine kinases – as a marker of myositis – was normalised. His symptoms improved and he went for clinical revalidation to regain condition.
DISCUSSION
Vasculitis
Constitutional symptoms and suspected myositis and mononeuritis multiplex were the main symptoms leading to small vessel vasculitis in this case. When vasculitis is considered, a detailed patient history and careful physical examination is essential, with regard to possible manifestations. Initial laboratory testing should include all tests presented in table 2, as well as eosinophil count, creatinine level, liver enzyme levels, and urinalysis.1,8 Depending on affected organs, specific tests such as electromyography or liquor tests can be performed. Vascular imaging through ultrasound, PET, CT, or MRI can support the diagnosis of large and medium vessel vasculitis.9 For small vessel vasculitis, histological examination is necessary to confirm diagnosis and can be best performed in an affected organ.8 Neutrophilic infiltration surrounding and involving blood vessel walls and fibrinoid necrosis are typical. Leucocytoclasia, extravasation of erythrocytes, necrosis, and thrombi can also be seen. The performed serum tests (auto-immune serology, complement factors, eosinophils) are necessary to differentiate in specific aetiology of vasculitis (table 3). However, a normal biopsy does not exclude vasculitis, as the inflammation can be segmented.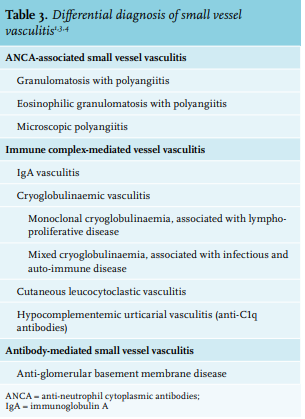
Cryoglobulinaemia
Cryoglobulinaemia is defined as the precipitation of immunoglobulins with cold temperature. Symptomatic cryoglobulinaemia is considered a rare disease in Europe,10 although exact prevalence is unknown due to the heterogeneity in cause, clinical presentation, and geographical distribution.11 After immunofixation, three subtypes can be identified.12 Solely monoclonal immunoglobulins (paraproteins) are referred to as type I; type II comprises both monoclonal and polyclonal immunoglobulins, and type III only polyclonal immunoglobulins. Due to overlapping clinical presentation and pathophysiology, type II and III are also referred to as mixed cryoglobulinaemia; 5-25% of cryoglobulins are monoclonal.13,14
The cryoprecipitability of monoclonal immunoglobulins depends on intrinsic factors such as pH, temperature, and absence of sialic acid moieties.1 The aggregated cryoglobulins seem to saturate the mononuclear phagocyte system activity, possibly by influencing Fc receptor function, resulting in accumulation and deposition of the cryoglobulins in specific organs.15 Clinical presentation of cryoglobulinaemia is divergent, and in most cases even asymptomatic.16,17 Symptoms are often secondary to hyperviscosity and vascular occlusion, such as Raynaud phenomenon, acrocyanosis, purpura, cold urticaria, ulcers, or skin necrosis.1 Leucocytoclastic vasculitis due to type I cryoglobulinaemia is rarely described. A French nationwide study identified 64 patients between 1995 and 2010; before that, only case reports with few patients were published. None of these patients reported typical vaso-occlusive symptoms.14
In contrast, leucocytoclastic vasculitis is typically seen in mixed cryoglobulinaemia.1 Immunoglobulins associate with rheumatoid factor (in contrast to monoclonal cryoglobulins), form immunocomplexes, and precipitate in small and medium-sized vessels. This leads through inflammation and complement activation to leucocytoclastic vasculitis. Mixed cryoglobulinaemia is related to chronic viral infections (particularly hepatitis C, but also associated with hepatitis B and HIV), autoimmune diseases, and lymphoproliferative disorders.18 Cryoglobulins could be detected in more than 50% of patients who were infected with chronic hepatitis C virus or HIV.19
The diagnostic approach of cryoglobulinaemia is focused on identifying involved organs and underlying disease, as this influences treatment decisions.1 Renal and/or skin involvement can be diagnosed with urinary analysis, renal, or skin biopsy.2,8 The type of cryoglobulinaemia has an important role in identifying underlying disease, and therefore quantity and type of immunoglobin and presence of rheumatoid factor should be determined. Type I cryoglobulinaemia is strongly associated with underlying lymphoproliferative disorder, such as Waldenström’s macroglobulinaemia or chronic lymphoid leukaemia.13 Therefore, bone marrow examination is indicated.
Level of paraprotein and severity of symptoms
As our case demonstrates, even a limited quantity of paraprotein can cause cryoglobulinaemia with severe symptoms. A recent retrospective study among 64 patients with type I cryoglobulinaemia could not identify a correlation between paraprotein level and clinical severity.20 Previous studies already demonstrated that the concentration of paraprotein has little or no prognostic value.1,21 Therefore, starting treatment against Waldenström’s macroglobulinaemia is based on symptoms, regardless of the paraprotein level. In the majority of patients with type I cryoglobulinaemia, treatment of underlying disease leads to improvement or stabilisation of symptoms.13
CONCLUSION
Vasculitis can be a presenting symptom of type I cryoglobulinaemia due to lymphoproliferative disease, although rarely seen. Vasculitis should be considered in patients with constitutional symptoms and symptoms of multiple affected organs. An extensive diagnostic process is necessary to identify underlying cause. This case emphasises that even very limited quantity of paraproteins can lead to cryoglobulinaemia with severe symptoms.
DISCLOSURES
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES