KEYWORDS
Encephalitis, lymphoma, rituximab
INTRODUCTION
Rituximab is an anti-CD20 monoclonal antibody which is widely used in CD20-positive B-cell-mediated diseases, including several auto-immune diseases and B-cell malignancies. In B-cell non-Hodgkin’s lymphomas (B-NHL), rituximab is the backbone of the therapy and in some types of B-NHL (low grade NHL and mantle cell lymphoma), maintenance treatment for 2-3 years is standard care. We present two patients treated with rituximab maintenance therapy who were diagnosed with a viral encephalitis.
CASE 1
The first case is a 66-year-old Caucasian female with a stage IV mantle cell lymphoma (MCL) diagnosed in 2008, with a relapse in 2017. Initial treatment consisted of three cycles of R-CHOP (rituximab, cyclophosphamide, adriamycin, vincristine, and prednisone), followed by two cycles of rituximab and cytarabine and consolidated with an autologous stem cell transplantation after BEAM (carmustine, etoposide, cytarabine, and melphalan) conditioning. The relapse nine years later was treated with rituximab-bendamustine. After six courses of rituximabbendamustine, a complete remission was achieved. Afterwards, the patient was scheduled for rituximab maintenance therapy (375 mg/m2) every three months.
After the first cycle of rituximab, she developed a headache and severe perceptual hearing loss in both ears resulting in deafness within two weeks. A course of prednisone did not improve her hearing. The neurological examination was unremarkable expect for an unsteady gait. On cerebral magnetic resonance imaging (MRI), there was neither evidence of lymphoma localisation nor other pathology in the cerebellopontine angle or trochlear nerve. The cerebrospinal fluid (CSF) was clear with a slightly elevated leucocyte count and protein level (table 1). 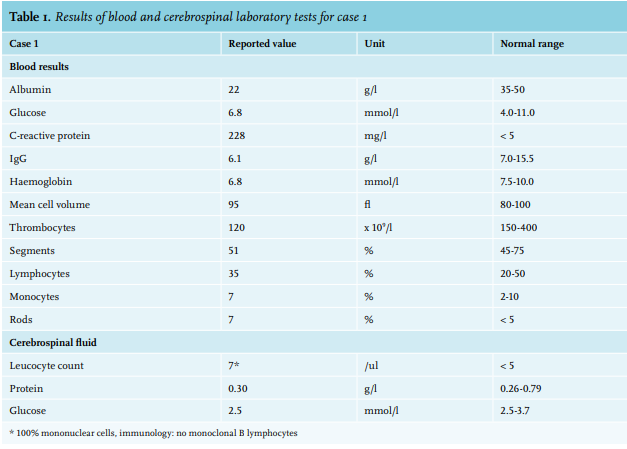
The polymerase chain reaction (PCR) of the CSF was positive for enterovirus DNA; C-reactive protein (CRP) was elevated; there were a leucopoenia and thrombocytopenia; and IgG was lowered (6.1 g/l; normal range 7.0-15.5 g/l). Both a computed tomography (CT) scan of the neck, thorax, and abdomen and a bone marrow biopsy demonstrated no evidence of residual MCL. There were not enough B cells present in the CSF to determine monoclonality. At presentation, the patient also had a fever without shortness of breath. On chest-X ray, a consolidation was seen, suspicious for pneumonia. Blood cultures, obtained before the start of antibiotics, were negative. A consolidation in the right lower lobe was seen, suspicious for pneumonia. The patient was therefore treated with a 5-day course of amoxicillin. Because the patient remained neurologically stable, and because her IgG was only slightly lowered and neutropenia was absent, no intravenous immunoglobulin (IVIG) was administered. The patient was scheduled for cochlear implants. Before cochlear implantation, the patient developed a new fever, atrial fibrillation, pleural effusions, peripheral edema, and diarrhoea with submucosal thickening of the ileum on CT. No evidence for MCL was found in the pleural effusion. Treatment consisted of broad-spectrum antibiotics and a 5-day course of IVIG (400 mg/kg). Despite these interventions and paramedical support by the physiotherapist and feeding by an enteral feeding tube, the physical condition of the patient gradually deteriorated. She developed rapidly changing blood pressures, became respiratory insufficient, and died several days later in the intensive care unit. No apparent cause was found for this sudden deterioration. Repeated blood, faeces, and urine cultures were negative. Pulmonary embolism was ruled out. After the patient died, the family did not give permission for autopsy.
CASE 2
The second case is a 73-year-old Caucasian male with a stage IVa low grade non-Hodgkin lymphoma diagnosed in 2016 with encasement of the thoracic aorta and mediastinal vessels. Treatment consisted of eight cycles of R-CVP (rituximab, cyclophosphamide, vincristine, and prednisone), after which, a partial response was achieved, followed by rituximab maintenance therapy every three months (375 mg/m2 ). After five cycles of rituximab maintenance therapy, the patient developed paroxysmal complaints consisting of nausea and light flashes in both eyes during several minutes, followed by apraxia and weakness in the right leg for half an hour with spontaneous resolution. The patient experienced several of these episodes during the week, often at the end of the day. Other complaints were a postural eadache. Neurological examination was normal except for symmetrical hyporeflexia of the upper extremities and an intentional tremor. Cerebral MRI did not show structural abnormalities. Because the complaints declined spontaneously, rituximab was continued. After the next cycle of rituximab, the paroxysmal complaints increased in frequency and severity. The headache increased and ataxia of the lower extremities was observed with a wide-based gait. The patient was mildly confused. A fever was also measured (38.5°C). Total gamma globulins were slightly lowered (5.7 g/l, normal range 6.0-13.7 g/l). Laboratory results are shown in table 2.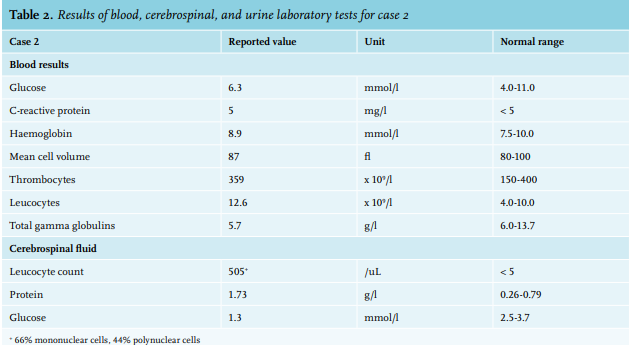
In the CSF, the leucocyte count was elevated with decreased glucose levels and elevated protein. There was no monoclonal cell population detected. CT and MRI of the brain did not reveal abnormalities expect for atrophy. Antibiotic treatment for bacterial meningitis was initiated. The CSF PCR was positive for parechovirus DNA, resulting in the final diagnosis of a viral meningoencephalitis, after which the antibiotics were stopped and a three-day course of IVIG (400 mg/kg) was started. The patient’s walking ability recovered completely and the he no longer needed a walking aid. The last two cycles of rituximab were cancelled. We consider vincristine to be an unlikely cause for the complaints because they started several months after the last dose of vincristine. A side effect of rituximab cannot be ruled out as the complaints increased after another dose of rituximab, however this treatment may also exacerbate a parechovirus encephalitis. Rituximab has also been associated with progressive multifocal leukoencephalopathy (PML); however, both a CT and MRI of the brain did not reveal abnormalities indicative of PML.
DISCUSSION
Rituximab is a CD20-specific antibody which targets B cells from the pre-B cell stage up to the pre-plasma cell. Immunoglobulin production is relatively unaffected if rituximab is applied shortly because plasma cells do not express CD20. Prolonged use of rituximab may however, result in decreased B-cell function that can contribute to the risk of non-neutropenic infections (e.g., viral encephalitis) other than bacterial sinopulmonary infections which are frequently seen in patients with a common variable immunodeficiency. However, gammaglobulins are a marker for B-cell function. Moreover, rituximab may result in a dose-dependent T-cell inactivation which may also increase the risk of other types of infection.1 In a systematic review, it was shown that the addition of rituximab to chemotherapy resulted in an improved survival without an increase in severe infections (relative risk of infections = 1.00; 95% confidence interval range 0.87 to 1.14).2 In a more recent single centre retrospective study of 211 patients, 39% of patients developed hypogammaglobulinaemia after rituximab-based treatment for B-cell lymphoma.3 In 15 patients, immunoglobulins were administered because of recurrent infections. Hypogammaglobulinaemia was more frequently seen in patients receiving rituximab maintenance therapy compared to rituximab-based (chemo)immunotherapy (54.2% vas 32.8%, p = 0.015). In another series, especially the combination of rituximab and fludarabine resulted in non-neutropenic infections due to hypogammaglobulinaemia.4 Parechovirus and enterovirus belong to the group of picornaviruses, small RNA viruses without an envelope. Enterovirus infections may present with a wide range of symptoms from an undifferentiated febrile illness to severe meningoencephalitis.5 Enteroviruses are responsible for 72% of the viral central nervous system (CNS) infections in adults and are generally associated with a relatively favourable outcome.6,7 Both the innate and adaptive immune system are activated following an enterovirus infection.8 However, when B-cell function is compromised, enterovirus infections may cause more severe disease. In patients with primary immunodeficiency, 50% mortality rates of non-polio enterovirus CNS meningoencephalitis have been described.9 Commonly, patients with enterovirus CNS infections are treated with IVIG. Grisiariu and colleagues report on 12 patients with viral encephalitis during rituximab treatment who received IVIG, of whom 5 died.10 However, other studies stated that there is currently no effective treatment for enterovirus CNS infection.9,11
CONCLUSION
Rituximab maintenance therapy improves the event-free survival of B-cell lymphoma. However, prolonged use of rituximab can result in severe non-neutropenic infections, which may be due to B-cell dysfunction, dose-dependent T-cell dysfunction and hypogammaglobulinaemia. In cases of neurologic complaints, one must be aware of viral encephalitis.
REFERENCES