KEYWORDS
Epidemiology, methylmalonic acid, muscle strength, NHANES, vitamin B12
INTRODUCTION
The recognition of symptomatic cobalamin (vitamin B12) deficiency poses several challenges. First, the spectrum of complaints may be diverse, and symptoms such as paraesthesia in the hands and feet, muscle cramps, dizziness, cognitive disturbances, ataxia, fatigue, and depression may vary considerably between patients.1-6 Second, the prevalence of anaemia in vitamin B12 deficiency is lower than anticipated3,7, and neurological signs often occur in the absence of anaemia.8 Third, serum B12 as a diagnostic test for tissue B12 deficiency may fail, as many people with such symptoms may have serum B12 concentrations above the lower population reference limit, which may cause individuals with relevant deficiency to be missed.9,10 In some people, this may be caused by the recent use of oral supplementation with multivitamins, high-dose oral vitamin B12 preparations or even B12-fortified energy drinks.11,12 Fourth, there is a poor correlation between serum B12 concentrations and complaints related to deficiency,3,5,13 and some people with serum B12 concentrations below the lower reference limit may not have symptoms or may have normal active B12 concentrations.14 Better information on the association between serum B12 concentrations and clinical symptoms is therefore warranted.
Yet, in daily practice, many general practitioners consider serum B12 concentrations within the reference interval for the population (i.e., 140-700 pmol/l) as proof of sufficiency, and possible complaints in this situation are determined to not be related to deficiency. Several authors have shown that many people with vitamin B12 deficiency would be overlooked by incorrectly using only total serum B12 concentrations as status marker.9,15,16 They therefore advocate measurement of one or more biomarkers, including methylmalonic acid (MMA), homocysteine (HCys), and/or holotranscobalamin in people with serum B12 concentrations in the grey zone of 140 to 300 pmol/l, in order to establish a possible diagnosis of deficiency.9,17-19 Vitamin B12 is a pivotal cofactor in various enzymatic systems, and its deficiency will influence enzymes such as methylmalonyl-CoA mutase (MCM) and methionine synthase. As a consequence, vitamin B12 deficiency may result in high concentrations of MMA and HCys.20 The sensitivity and specificity of elevated MMA concentrations as an indicator of symptomatic B12 deficiency are unknown. Earlier studies have even suggested that MMA concentrations are a poor predictor of symptom score or neurological complaints.21 In addition, MMA concentrations may be elevated in people with severely impaired renal function.22,23 Chronic kidney disease and impaired renal function are associated with more comorbidity and a higher risk of frailty, and there is evidence that chronic kidney disease is linked with impairments of physical and cognitive function and quality of life.24,25 Similarly, elevated HCys concentrations may suggest symptomatic B12 deficiency, but HCys is also elevated in cases of folate deficiency or impaired renal function. Thus, although elevated MMA and HCys concentrations may be indicative of vitamin B12 deficiency, normal concentrations of these biomarkers do not rule out deficiency26 or a favourable response to cobalamin therapy.9 There are few large-scale studies that have reported on the association between serum B12, MMA, and functional status in the general population. A study in people > 70 years in Sweden showed that half of them had abnormal MMA or homocysteine concentrations, suggesting a latent or overt tissue deficiency of cobalamin or folate.11 The 2001-2002 and 2003-2004 National Health and Nutrition Examination Survey (NHANES), a long-term epidemiologic survey in the USA,27 showed that there is a large intermediate group of people whose B12 status is difficult to interpret.20 In NHANES participants > 60 years, vitamin B12 deficiency was associated with an almost 10-fold increased risk in peripheral neuropathy and a 20-fold increased risk of total disability.3 NHANES-based population reference values for MMA showed an age-related increase, due to both a gradual decline in kidney function with ageing, as well as vitamin B12 status.28
We combined data from two consecutive NHANES surveys of 2011-2012 and 2013-2014 in order to evaluate the association between serum B12 and MMA with haematological parameters and physical and cognitive functioning parameters. Furthermore, we also aimed to study the potential role of variation in serum B12 and MMA concentrations due to age and renal function on these associations.
MATERIALS AND METHODS
NHANES structure and inclusions
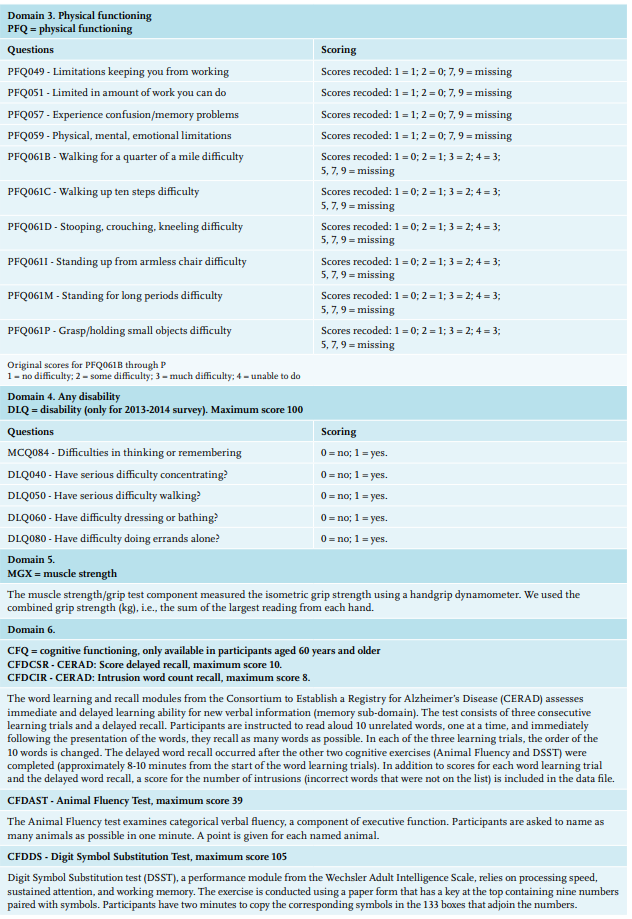
In short, NHANES is a cross-sectional survey in the U.S. that uses a complex, stratified, multistage probability sampling design.20,27 NHANES has obtained written informed consent from all participants. The survey protocol was approved by the Research Ethics Review Board of the National Center for Health Statistics, Centers for Disease Control and Prevention. Interview questionnaires and examination response rates are publicly available.29 Participants were first interviewed in their homes, during which demographic information and a variety of health-related information were collected. One to two weeks later, they underwent a standardised physical examination, as well as additional investigations such as exercise testing, 24-hour (h) dietary recall, and a blood draw in a mobile examination centre. Blood samples were taken with the participant fasting. Participants who visited the examination in the morning were requested to fast for nine hours; those visiting in the afternoon or evening were requested to fast for six hours. For this study, we created a dataset of NHANES 2011-2012 and 2013-2014 participants who were older than 19 years and had available serum B12 measurements. The NHANES survey included people from several ethnicities and the sample design for NHANES 2011-14 included an oversample of Asian Americans.
Outcomes
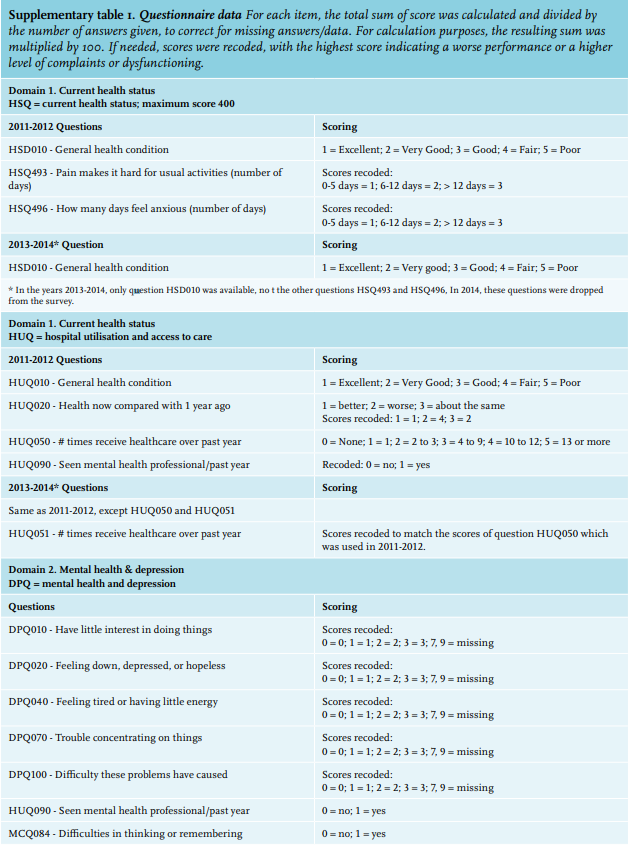
To estimate clinical complaints and functioning, we used data from the following NHANES questionnaires: current health condition, disability, hospital utilisation, medical conditions, cognitive functioning, mental health and depression, and physical functioning (supplementary table 1). Based on these questionnaires, we calculated symptom scores for current health status, mental health and depression, and physical functioning and disability, taking into account the most relevant questions/variables for each entity, as described in supplementary table 1. A higher symptom score conforms to a higher number of symptoms, complaints, and disturbance of functioning. We also evaluated the results of muscle strength which was measured through a grip test using a handgrip dynamometer as a separate parameter of physical functioning, and the results of cognitive functioning tests (the CERAD Word Learning sub-test, the Animal Fluency test, and the Digit Symbol Substitution Test (DSST), for details see supplementary table 1). The latter tests were only performed in participants aged 60 years and older. Reference values were calculated for participants who could be considered ‘healthy’, i.e., defined as those participants with serum B12 between 301 and 1000 pmol/l, normal serum MMA, estimated glomerular filtration rate (eGFR) > 60, and no medication use.
Exposures
Haemoglobin and mean corpuscular volume (MCV) measurement were performed with a Beckman Coulter MAXM for 2011-2012 and the Beckman Coulter DxH 800 for 2013-2014 (Beckman Coulter Inc, Brea, CA, USA). No significant trend changes for haemoglobin and MCV were reported from NHANES 2011-2012 to NHANES 2013-2014. Serum B12 concentrations were measured with electrochemiluminescence immunoassay on a Modular Analytics E170® system (Roche Diagnostics, Indianapolis, IN). Serum MMA concentrations were analysed by LC-MS/ MS as dibutylester after extraction from serum with tert-butylmethylether and derivatisation with butanol.30 Serum creatinine was measured with the Jaffe rate method (kinetic alkaline picrate) on a Beckman Synchron DxC800 modular chemistry analyser. All information regarding these methods are publicly available on the NHANES website.20,31
On the basis of serum B12 concentrations, three groups were constructed: 1) probable vitamin B12 deficiency, defined as a serum B12 concentration < 140 pmol/l; 2) ’possible deficiency’, serum B12 concentrations between 140 and 300 pmol/l; 3) normal concentrations, serum B12 > 300 pmol/l. Serum B12 concentrations greater than 1000 pmol/l were considered suggestive for supplementation with (parenteral) B12-containing preparations, and these participants were not included in the calculations. Serum MMA concentration ≥ 300 nmol/l was considered elevated. Anaemia was defined according to the World Health Organization criteria: haemoglobin concentration in men < 8.0 mmol/l and in women < 7.5 mmol/l, with MCV > 100 fl used as a definition for increased MCV.
Other variables
Medication use was scored in NHANES by the unique generic drug code from the Multum Lexicon Drug Database. The number of different medications reported by a participant was considered as a proxy for comorbidity.32 Current smoking was defined as a positive answer to question SMQ690A/691A: Have you used tobacco/nicotine during the last 5 days? Renal function was calculated as eGFR with the formula developed by the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI).33 Impaired renal function influences MMA concentrations, and thereby the prognostic influence of elevated MMA concentrations may be different in people with impaired renal function. Also, impaired renal function itself is associated with more comorbidity and a higher risk of frailty.24,25
Statistics
Functional outcomes were assessed in relation to serum B12 and MMA concentrations. We calculated all variables for the entire population of participants > 19 years of age, and separately for people from Western European descent (described in NHANES as Non-Hispanic Whites, supplementary table 2) to evaluate for generalisability to Dutch individuals. Means were compared between groups with analysis of variance. When variables were not normally distributed, medians were compared with the nonparametric Mann-Whitney U or Kruskal Wallis test. Chi-square test was used to analyse categorical variables. Univariable and multivariable linear regression analyses were performed to examine the association between relevant factors like serum B12 and MMA concentrations (both log transformed) and muscle strength. As age, sex, haemoglobin, serum creatinine (both log transformed), current smoking, and comorbidity are strong determinants of physical functioning and have been included in the multivariable model as co-factors.
NHANES has created specific sampling weights to account for its complex survey design (including oversampling), survey non-response, and post-stratification.34 The incorporation of sampling weights into estimated regression coefficients helps protect against the potential existence of missing regressors. In addition, the linearisation variance estimator is suggested to be robust against the likelihood of correlated errors and the possibility of heteroscedasticity.35,36 Although we did not intend to extrapolate our findings to the U.S. civilian non-institutionalised census population, we calculated our multivariable regression models with application of these weights. A p-value < 0.01 was used as a cut-off for statistical significance. Analyses were conducted using IBM SPSS Statistics (Version 24, IBM, Armonk, NY, USA) and Stata Statistical Software (version 16.0; Stata Corp).
RESULTS
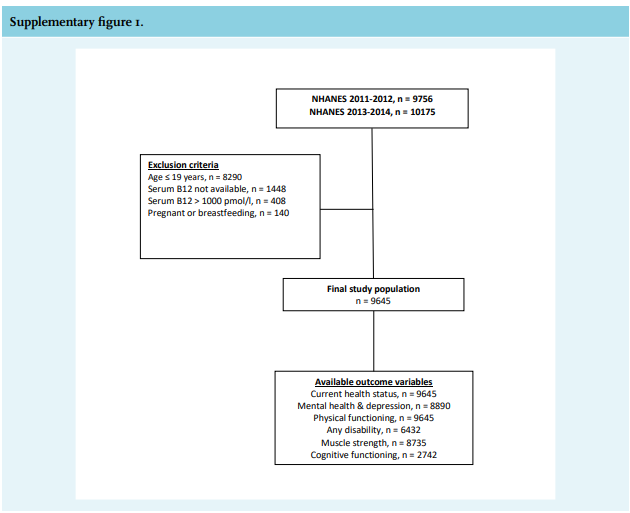
NHANES 2011-2014 included 19931 participants. A total of 10286 participants were excluded because of age ≤ 18 years, unavailability of serum B12 measurements, serum B12 > 1000 pmol/l, pregnancy or breastfeeding (supplementary figure 1). The final study population included 9645 participants with a mean age of 49 (standard deviation (SD) 17) years; 50.1% were males. Mean haemoglobin was 8.7 (SD 1.0) mmol/l (in men: 9.2 ± 0.8 mmol/l, in women 8.2 ± 0.8 mmol/l), eGFR 96 (SD 24) ml/min, and median serum vitamin B12 concentrations and MMA concentrations were 377 pmol/l (IQR 280-509) and 140 nmol/l (IQR 108-189), respectively. In total, 159 (1.6%) participants had serum B12 concentrations < 140 pmol/l, while 2760 (28.6%) had concentrations between 140 and 300 pmol/l. Of those participants with serum B12 < 140 pmol/l, 56.2% had elevated MMA concentrations, while only 4.4% had elevated MCV (table 1).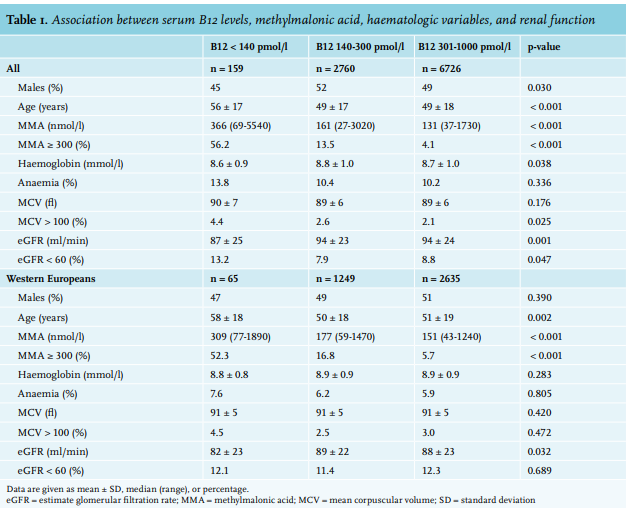
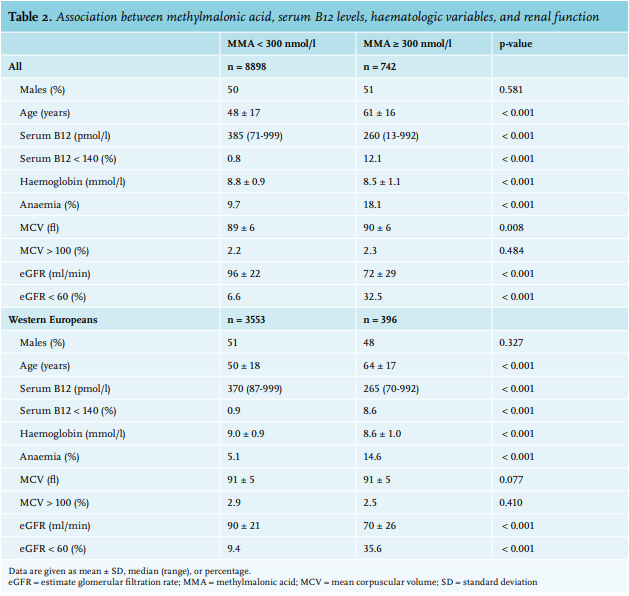
In those with serum B12 < 100 pmol/l, only 32 of 42 (76.2%) had elevated MMA concentrations. In participants with serum B12 in the grey zone between 140 and 300 pmol/l, 13.5% had elevated MMA, while this was 4.1% in subjects considered to have normal serum B12 (301-1000 pmol/l). Similar results were obtained when only participants of Western European descent were studied. In these, only half (52.3%) had elevated MMA when serum B12 was < 140 pmol/l. Elevated MMA concentrations ≥ 300 nmol/l (table 2) were associated with significantly lower serum B12 and haemoglobin concentrations, and lower eGFR, but not with MCV or percentage of participants with elevated MCV.
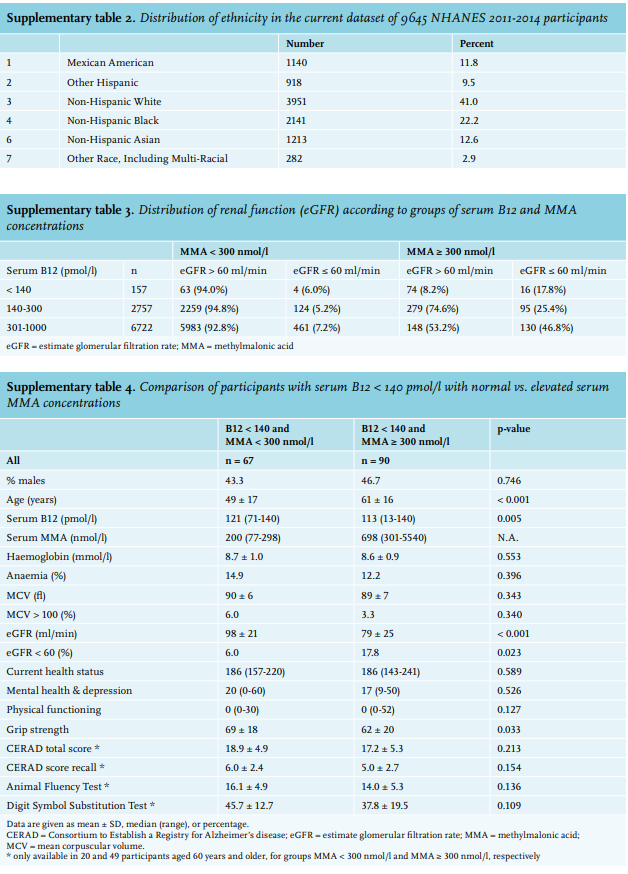
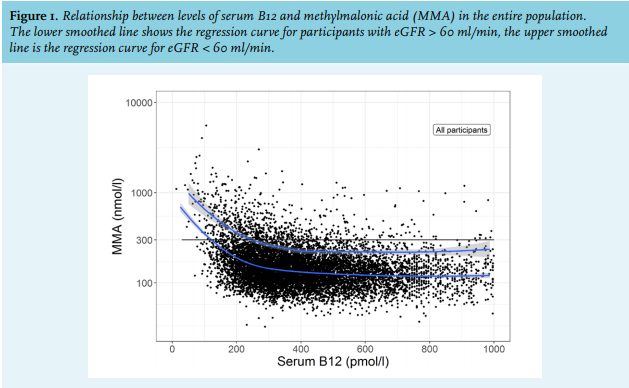
There was a curvilinear association of serum B12 with MMA by which lower serum B12 was associated with higher MMA (figure 1). Elevated concentrations of MMA can be found across the entire spectrum of serum B12 concentrations (figure 1). Participants with an eGFR < 60 ml/min had a higher MMA for a given serum B12 concentration. In participants with serum B12 < 140 pmol/l, we identified that 43.8% had a normal MMA concentration (table 1). In participants with serum B12 in the grey zone and elevated MMA concentrations, 25.4% had an eGFR ≥ 60 ml/min, whereas in those with serum B12 between 301 and 1000 pmol/l, 46.8% of those with elevated MMA had an eGFR < 60 ml/min (supplementary table 3). Impaired renal function was found in 5.2-7.2% participants with normal serum MMA (supplementary table 3).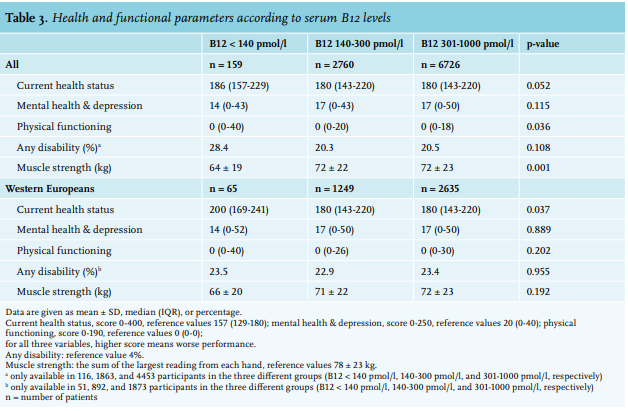
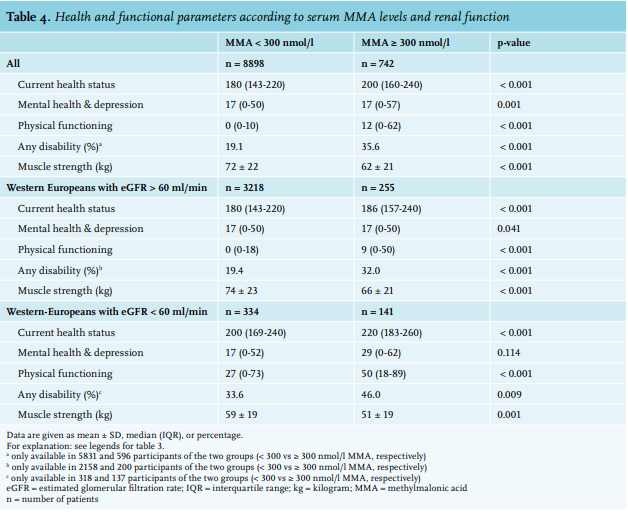
Participants with serum B12 < 140 pmol/l reported significantly worse physical functioning and had lower muscle strength compared to those with serum B12 levels between 140-300 pmol/l and > 300 pmol/l (table 3). Both differences were lost when only people of Western European descent were evaluated. In the total population and in Western Europeans, we observed a significantly lower score in all functional outcomes, including muscle strength, for those with MMA concentrations > 300 nmol/l in comparison with people with normal MMA concentrations (table 4). In order to correct for impaired renal function, we re-calculated the composite outcomes and muscle strength for participants with an eGFR > 60 ml/min. Again, we observed lower performance with MMA ≥ 300 nmol/l, but the overall scores were slightly better for participants with an eGFR > 60 compared to those with an eGFR < 60 ml/min.
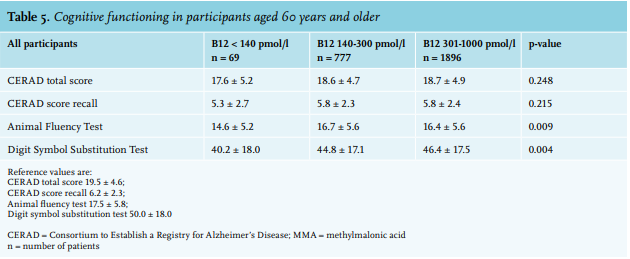
Table 5 shows the results of the cognitive function tests for all participants aged 60 years and older. The participants with serum B12 < 140 pmol/l had a lower score on the Animal Fluency Test and the Digit Symbol Substitution Test, compared to participants in the other groups, whereas the scores on the CERAD Word Learning and Recall test were similar. Participants with MMA ≥ 300 nmol/l had a lower score on all domains. Scores for the Intrusion Word Count were not different between the groups; 20.7% of participants with normal MMA compared with 19.5% with elevated MMA produced one or more intrusion words. Similar results were obtained for participants of Western European descent. Participants with normal renal function had significantly better score (p < 0.001 for all three domains) compared to those with impaired renal function. Comparison of participants with serum B12 < 140 pmol/l with normal or with elevated serum MMA concentrations showed that those with MMA ≥ 300 nmol/l were older, had slightly lower median serum B12 concentrations and more frequently impaired renal function; their haemoglobin, MCV concentrations and functional status were not different. Although the cognitive function tests showed lower scores for those with elevated MMA, these differences were not statistically significant due to low numbers (supplementary table 4).
Serum B12 concentration (log transformed) was not significantly associated with muscle strength (coefficient -0.279, SE 0.82, p = 0.737), while serum MMA (log transformed) was significantly associated with muscle strength (coefficient -6.90, SE 0.79, p < 0.001). The results of the multivariable regression analyses for muscle strength are depicted in table 6. For the entire population, we observed a significant and independent contribution for gender, age, and MMA concentrations, as well as haemoglobin concentrations and co-morbidity. Serum B12 was not independently associated with muscle strength. Similarly, age, serum B12, MMA concentrations, and co-morbidity were independently associated with the physical functioning symptom score, whereas only age and co-morbidity were significantly associated with current health status and mental health.
D I S C U S S I O N
In this study, we have shown that a large proportion of individuals with a decreased serum B12 concentration still has normal MMA concentrations. In addition, in people with serum B12 concentrations in the grey zone between 140 and 300 pmol/l, 13.5% had elevated MMA concentrations. Only a very small proportion of participants with low serum B12 and elevated MMA had anaemia, with or without elevated MCV. Participants with serum B12 concentrations < 140 pmol/l had lower physical functioning and muscle strength in the entire population, but not in the subgroup of participants of Western European descent. Serum MMA concentrations were strongly associated with all clinical outcomes and with muscle strength in both the total population as well as participants of Western European descent.
When evaluating the functional status or performance of the participants, serum MMA concentrations proved to be a better indicator of poor functional status than serum B12 concentrations. In all domains, participants with elevated MMA ≥ 300 nmol/l had worse scores compared to those with MMA < 300 nmol/l. This is confirmed in our evaluation of muscle strength as a functional marker. Regression analysis showed that MMA, but not serum B12, was a significant and independent predictor of muscle strength in all subpopulations evaluated; i.e., the entire population, participants of Western European descent, and those with normal renal function. In an earlier study in NHANES participants > 60 years, it was demonstrated that vitamin B12 deficiency was associated with an almost 10-fold increased risk in peripheral neuropathy for participants with serum B12 < 200 pmol/l and homocysteine > 20 µmol/l, but only a 1.4 fold increase for participants with B12 (< 258 pmol/l) or MMA (> 210 nmol/l).3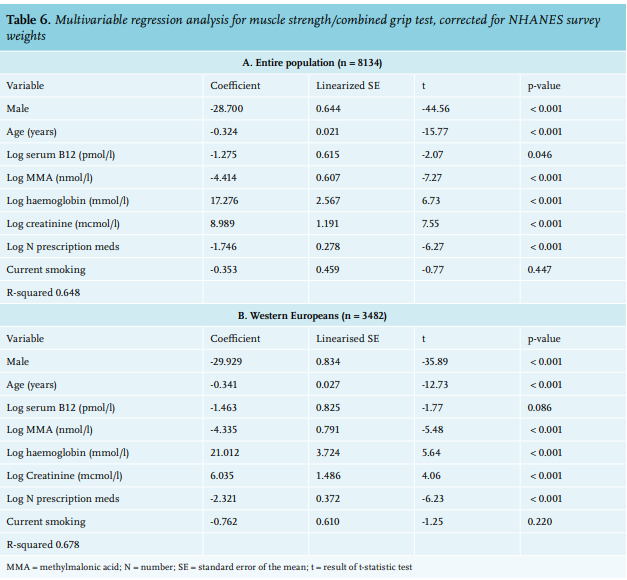
We aimed to investigate cognitive domains in relation to serum B12 and MMA concentrations. As shown in tables 3, 4, and 6, elevated MMA concentrations were more strongly associated with poor functional performance than serum B12. There is limited literature on the relationship between serum B12, its biomarkers, and cognitive performance. Hooshmand et al. reported that higher serum homocysteine concentrations were associated with poorer performance in global cognition, memory, executive functions, and verbal expression, while higher baseline holotranscobalamin (holoTC) was significantly associated with better performance in global cognition, executive functioning, and psychomotor speed.37 In the Maine-Syracuse study, serum B12 concentrations and total homocysteine concentrations were positively and negatively associated, respectively, with cognitive performance.38 Lewis et al. reported that elevated MMA concentrations appeared to be more reflective of cognitive impairment than serum B12, even when corrected for serum creatinine concentreations,39 and similarly, high plasma homocysteine and serum MMA concentrations correlated inversely with movement and cognitive performance.40 Taken together, these studies support our observation that biomarkers show a stronger association with functional outcome than serum B12 measurements. A study in people aged 75 and above showed that serum folate concentration was a more important determinant of cognitive performance than serum B12.41 The results of this observational study are of clinical importance for our approach towards patients with presumed or possible vitamin B12 deficiency. Some clinicians and clinical chemists consider elevated MMA as the single proof of existing B12 deficiency, and they base their diagnostic algorithms on this. However, almost 25% of people with serum B12 concentrations < 100 pmol/l had normal MMA concentrations. This has been previously observed: approximately 63% of people with low holo-transcobalamin (holoTc) levels < 20 pmol/l, indicative of true deficiency, had normal serum MMA concentrations.26 This supports observations that serum MMA is not a very sensitive indicator of tissue B12 deficiency. Indeed, Schrempf W. et al. reported that both serum B12 and holoTC levels were weak predictors of abnormal MMA levels.15 Other studies have confirmed that normal levels of MMA may be measured even in situations of very low B12 levels.42 In addition, there are isolated reports showing that serum B12, homocysteine, and MMA levels are unreliable predictors of B12-responsive neurological disorders.43
The curvilinear association between serum B12 and MMA has been shown by Bailey et al. 20 in an earlier subset of NHANES participants, combining all available data from three consecutive NHANES screenings (1999-2000, 2001-2002, 2003-2004). These authors also showed that for each level of serum B12, MMA concentrations were higher in groups of participants with higher age.20 Possibly, reductions in eGFR may mediate some of these differences, and they also raise the question whether age-specific reference values for MMA should be used.23 This is supported by the observation that eGFR is independently associated with MMA in multivariable analysis. In the current paper, we confirmed that a serum B12 within the normal reference range, i.e., > 140 pmol/l, does not definitively reflect normal tissue B12 activity as estimated by serum MMA concentrations. This is also supported by our regression analysis, as depicted in figure 1, where the curvilinear course has an inflection point between 300 and 400 pmol/l of vitamin B12. This clearly supports the assumption that the area of vitamin B12 insufficiency extends above the lower reference value of serum vitamin B12.
Clinicians must consider that an impairment in renal function may increase serum MMA concentrations. As shown, NHANES participants with impaired renal function (eGFR < 60 ml/min) had poorer functional outcomes compared to those with an eGFR above 60 ml/ min. A recent publication has provided information on how to adjust serum MMA concentrations for a reduction in eGFR in people with serum B12 levels between 90 and 300 pmol/l, and these calculations were intended to reduce the number of patients classified as vitamin B12 deficient.23 However, based on the current data (table 1 and supplementary table 4), as well as earlier observations, serum MMA below 300 nmol/l does not exclude vitamin B12 deficiency.15,26
Classically, vitamin B12 deficiency has been associated with macrocytic anaemia. However, neurological signs of vitamin B12 deficiency are often present in the absence of anaemia.8 The prevalence of anaemia in vitamin B12 deficiency appears to be lower than anticipated.7 In NHANES participants, fewer than 10% of people considered to be vitamin B12 deficient had macrocytosis.3 In the current study, the number of people with serum B12 < 140 pmol/l and anaemia and/or elevated MCV is small: anaemia was observed in 13.8% of these participants and elevated MCV in 4.4%. Prevalence of anaemia in those with MMA ≥ 300 nmol/l was 18.1%. Causes of anaemia may be complex and concomitant iron deficiency may mask macrocytosis.44 It should be noted however, that we currently report data from an epidemiological survey and not data regarding patients referred for suspected vitamin B12 deficiency. In the latter group, prevalence of anaemia may be higher. Nevertheless, as anaemia is only seen in a minority of patients with vitamin B12 deficiency, its absence should not be considered as proof that vitamin B12 status is normal.
The results of the current study may help clinicians to identify pitfalls in diagnosing vitamin B12 deficiency. First, since 13.5% of these people with serum B12 concentrations > 140 and < 300 pmol/l have elevated MMA provides evidence that such serum B12 concentrations should not always be interpreted as normal, which is in accordance with several earlier reports.6,9,15,19 Second, serum MMA is not a sensitive marker; the high percentage of people with low serum B12 but normal MMA suggests that the prevalence of tissue B12 deficiency may even be higher than can be estimated based on abnormal serum MMA concentrations. As the natural course of vitamin B12 deficiency is not well-known, it cannot be excluded that participants with low serum B12 but normal MMA may be in the early, still asymptomatic phase of their deficiency.45 Earlier studies have shown the importance of treatment response. In one of his papers, Solomon concluded that if cobalamin therapy had been restricted to symptomatic patients with both low or intermediate serum B12 concentrations and increased MMA or homocysteine concentrations, 63% of responders would not have been treated.9 Functional vitamin B12 deficiency can be present in patients with apparently normal serum B12 concentrations, either related to defects in intracellular transport of B12,46 due to interference of serum B12 assays by intrinsic factor antibodies,47-51 or by masking due to the use of oral vitamin B12-containing supplements.11,12 The high prevalence of elevated MMA in people with serum B12 > 140 pmol/l refutes the proposed algorithm for cost minimisation which was reported in this journal in 2013.52 Applying the proposed algorithm will therefore, leave several people undiagnosed, who do have a high probability of vitamin B12 deficiency. Taken together, there is a great need of a generally accepted definition of vitamin B12 deficiency, which takes into account complaints, baseline biochemical results, and response to treatment.9 Most studies have until now focus on normalisation of serum B12 or MMA, and do not specifically address the clinical syndrome, complaints, or quality of life.6,53
Strengths and limitations
This study was adequately powered to study the associations of interest, because we used a large NHANES dataset that reflects the general U.S. population. In addition, we considered potential effects of renal function and age, and have been able to provide sub-analyses in participants of Western European descent to evaluate for generalisability to Dutch individuals. Earlier studies have suggested that ethnicity may influence this association.20 Because of its cross-sectional nature, we cannot be sure that the same results will apply to patients who are evaluated because of specific (neurological) complaints and are found to have low serum B12 concentrations. In NHANES 2011-2012 and 2013-2014, no direct assessment of peripheral neuropathy was available. The observational nature of this study does not allow for conclusions regarding causality. Also, the use of the NHANES dataset could limit the generalisability to the Dutch population.
CONCLUSIONS
MMA concentrations are elevated in only 56% of people with serum B12 concentrations < 140 pmol/l, and in 13.5% of people with serum B12 in the grey zone of 140-300 pmol/l. MMA concentrations proved to be a more reliable predictor of complaints, functional status, and physical performance than serum B12. Measuring serum MMA may also assist with diagnosing tissue B12 deficiency in cases of doubt when serum B12 concentrations are higher than 140 pmol/l, but this biomarker may also be elevated in people with (severely) impaired renal function.
DISCLOSURES
Acknowledgements
We thank the data collection team and NHANES administration and staff for the data and reports made available through the NHANES website that allowed us to generate this paper.
Availability of data and material
We used publicly available and de-identified NHANES data collected by the National Center for Health Statistics, Centers for Disease Control and Prevention for the present study. https://www.cdc.gov/nchs/nhanes/index.htm
Funding
This analysis was supported by the National Consortium for Healthy Ageing, and funds from the European Union’s Seventh Framework program (FP7/2007-2013) through the BioSHaRE-EU (Biobank Standardisation and Harmonisation for Research Excellence in the European Union) project, grant agreement 261433.
Conflicts of interest
All authors declare no conflicts of interest.
REFERENCES
A P P E N D I X