KEYWORDS 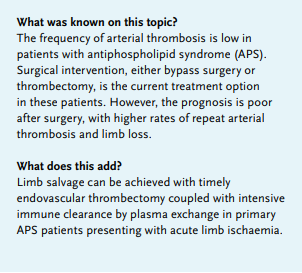
Acute limb ischaemia, antiphospholipid syndrome, endovascular thrombectomy, plasma exchange
INTRODUCTION
Antiphospholipid syndrome (APS) is an autoimmune disease characterized by cardinal manifestations of venous or arterial thrombosis and/or obstetric complications in the presence of antiphospholipid antibodies known as lupus anticoagulants (LAC), anticardiolipin antibodies, and antibodies against β2-glycoprotein 1.1,2 Although the frequency of arterial thrombosis in the lower limbs is low in APS patients,3 limb prognosis is poor, and the majority of patients eventually require minor or major amputations to prevent disease progression and mortality.4 Surgical intervention, either bypass surgery or thrombectomy, has been the treatment option for acute limb ischaemia (ALI) in APS patients for the past few decades. However, reported rates of arterial thrombosis and limb loss post-operation were 50-91% and 43%, respectively.5-7 Recently, endovascular therapy (EVT), with either catheter-directed thrombolysis (CDT) or thrombectomy devices, has become the first-line therapy for ALI patients. We report a case of APS complicated by repetitive arterial thrombosis, and demonstrate the efficacy of combined EVT and plasma exchange in rescuing the threatened limb. 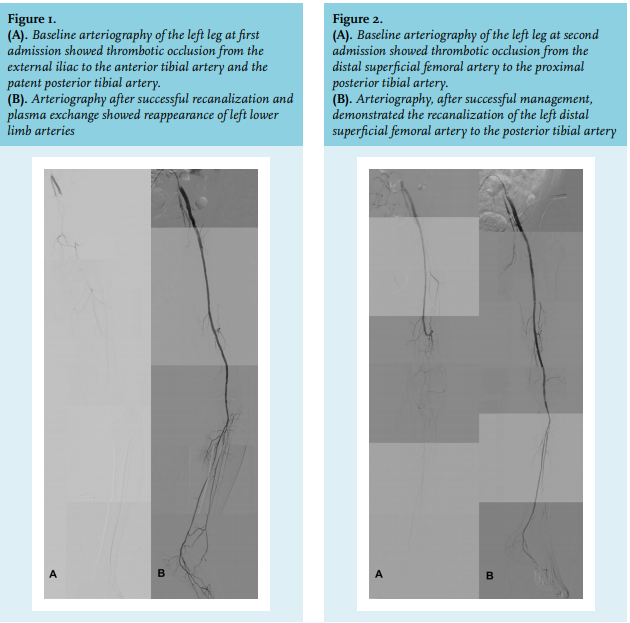
CASE REPORT
A 42-year-old man was referred to our institution for resting pain and coldness in his left leg, which had persisted for several days. He was a non-smoker with no known risk factors for atherosclerosis, including diabetes mellitus, hyperlipidaemia, hypertension, or a premature family history of cardiovascular events. On admission, physical examination revealed coldness, livedo reticularis, the absence of pulsation in the left infra-inguinal arteries, and left foot drop. Duplex ultrasound showed thrombotic occlusion of the common femoral artery (CFA) to the anterior tibial artery, and patent left posterior tibial artery (PTA). Serologic tests were negative for all of the following: antinuclear antibody, anti-dsDNA antibody, anti-ENA antibody, antineutrophil cytoplasmic antibody, rheumatoid factors, complement C3 and C4, cardiolipin immunoglobulin G and immunoglobulin M, and anti-β2-glycoprotein 1 antibody. The test-to-control plasma ratio of LAC was positive in both screening (4.19; ≤ 1.20 for negative test) and confirmatory tests (2.45; > 1.2 for a positive test), as determined by the dilute Russell’s viper venom time (dRVVT). Antithrombin III, protein C, and protein S levels were normal.
We performed diagnostic angiography via the right CFA with the cross-over approach, which showed complete thrombotic occlusion from the left external iliac artery (EIA) to the foot vessel with patent PTA only (figure 1A). After wire crossing, we performed pre-dilatation with a low-profile balloon followed by intravascular ultrasound assessment (Volcano, Visions PV 0.018, CA, USA), which was aligned with a thrombus-containing lesion between the EIA and the proximal PTA. Mechanical thrombectomy was performed using a Rotarex®S thrombectomy system (Straub Medical AG, Wangs, Switzerland), followed by balloon angioplasty from the EIA to PTA. Continued urokinase was administered via infusion catheter to treat residual thrombus, but the vessel repeatedly occluded. We performed another mechanical thrombectomy using the AngioJet thrombectomy system (Bayer Medical, Minneapolis, MN, USA) to treat the distal popliteal artery and proximal PTA. After successful restoration of direct flow to the foot, hydroxychloroquine and steroid therapy with methylprednisolone (80 mg per day) were administered to achieve immunosuppression of APS. In addition, four sessions of plasma exchange with fresh frozen plasma (FFP) as the replacement fluid were performed on alternate days for immune clearance. This reduced the thrombogenicity of LAC. The patient was successfully discharged one week later with a patent vessel after the treatment mentioned above (figure 1B). The discharge medications included dabigatran (150 mg) and hydroxychloroquine (200 mg) twice a day.
Two weeks post-discharge, symptoms in the left leg reoccurred, and angiography showed occlusion of the left distal superficial femoral artery and popliteal artery (figure 2A). We repeated EVT and administered 11 sessions of plasma exchange with FFP (consecutive sessions for the first three days, followed by eight sessions, performed on alternative days) to salvage this leg. Reintervention and removal of the LAC by plasma exchange freed the patient from recurrent thrombosis and restored direct flow to the left foot (figure 2B).
After discharge, we administered a total dose of 1000 mg rituximab (Roche, Basel, Switzerland) over a 2-week period, and maintained the following medications: dabigatran, ticagrelor, hydroxychloroquine, and prednisolone. The repeated test-to-control plasma ratio of LAC performed was still positive in both screen and confirmatory tests four months after the first episode, which confirmed the diagnosis of antiphospholipid syndrome according to the revised Sapporo criteria.8 The patient was free from further thrombotic events over the next eight months, and duplex ultrasound showed sustained patency from the iliofemoral artery to the lateral plantar artery.
DISCUSSION
Although the incidence of ALI in patients with primary APS is rare, the prognosis for limb salvage is poor, with the majority of patients eventually undergoing major or minor amputations.4 Previous studies reported a higher rate of postoperative thrombotic complications in patients with APS who underwent surgical treatment, especially for vascular procedures.5,6 Ciocca et al. confirmed this extreme postoperative thrombotic rate.7 Of 19 patients positive for antiphospholipid antibodies and undergoing surgical procedures for cardiovascular disease, 16 had postoperative complications, in particular, arterial thrombosis, and 12 died of complications related to surgery. Some authors postulated that damage to the endothelial cells of the vessels during manipulation might precipitate or aggravate the pre-existing susceptibility to thrombosis.9
EVT, a minimally invasive and reproducible procedure, has recently become the treatment of choice for patients with ALI. In this case, timely EVT averted irreversible tissue damage due to acute arterial occlusion. Plasma exchange was performed soon after restoration of the blood flow, aiming to remove antiphospholipid antibodies, cytokines, and complement to achieve a clean slate status. Nevertheless, repetition of thrombotic occlusions occurred two weeks post-discharge, suggesting that inadequate autoantibody clearance and procedure-related endothelial damage might induce further thrombus formation in patients with hypercoagulability status. During the second episode, removal of autoantibodies by intensive plasma exchange attenuated the hyper-response of the coagulation cascade. In addition to steroid and hydroxychloroquine treatment, rituximab was used to further suppress the hypercoagulability status.
This case highlights the feasibility of timely endovascular thrombectomy, coupled with intensive immune clearance after post-plasma exchange, for limb salvage in primary APS patients presenting with ALI. However, effective immunosuppression and appropriate anticoagulation are essential to prevent recurrent thrombotic events.
DISCLOSURE
All authors declare no conflicts of interest. No funding or financial support was received.
REFERENCES