KEYWORDS
Urinary tract infections, emergency departments, antibiotic resistance
INTRODUCTION
Background and rationale Urinary tract infection (UTI) is suspected in a substantial group of patients visiting the emergency department (ED). In the United States, UTIs accounted for approximately 2% of ED visits in 2014 for a total of 2.3 million people.1 This percentage is similar in the Netherlands.2 There is continuous debate about the appropriate antibiotic treatment for patients with UTI, despite guidelines on the subject. The Dutch guidelines for antibiotic therapy are based on national resistance data on pathogens causing UTI.3 It is questionable if, and to what extent, these data are applicable to the patient population encountered in specialized hospitals, such as university hospitals.
Patients in university hospitals often have a complex medical history and in particular, patients from nephrology and urology departments are more frequently treated for UTIs with antibiotics. These patients are at risk for colonization with antibiotic-resistant uropathogens. When UTI occurs, it is likely that the uropathogens are less susceptible to routinely prescribed antibiotics.4-6 Data comparing the distribution and antibiotic susceptibility of uropathogens in Dutch university hospitals with the overall distribution in the Netherlands are currently lacking.
Dutch national guidelines advise to treat complicated UTIs (cUTI) with amoxicillin or a second-generation cephalosporin combined with an aminoglycoside, or with a third-generation cephalosporin.3 A cUTI is defined by the ‘The Dutch Working Party on Antibiotic Policy’ (SWAB) as all UTIs with the exception of cystitis in non-immunocompromised, non-pregnant women with no anatomical and functional abnormalities of the urogenital tract and no signs of tissue invasion, and in men younger than 40 years without a medical history, no previous lower urinary tract symptoms and no findings at physical examination.3 In the Erasmus University Medical Center Rotterdam, the Netherlands (Erasmus MC), cefuroxime combined with gentamicin is the antibiotic regimen of choice for cUTI based on local resistance data. This regimen can only be administrated intravenously, which requires hospitalisation, regardless of the patient’s clinical condition. Furthermore, side effects of gentamicin include nephrotoxicity and ototoxicity.7 Although this risk is particularly applicable after multiple doses in patients with renal insufficiency, aminoglycosides are frequently left out, resulting in inappropriate treatment.8-10 The duration of hospital stay or even prevention of admission may be achieved if hospitals can identify patients who can be safely treated with other specific antibiotic-regimens, based on their medical history and available data from previously obtained cultures.
When initiating adequate antibiotic therapy, physicians should take the increase of antibiotic resistance into account. However, there are currently not enough data to enable a more tailor-made decision for the first choice of the antibiotic regimen. Recently, a study in a university hospital in Israel showed that patients who had a culture with a resistant uropathogen had high rates of a repeat resistant uropathogen in a subsequent culture.11 This chance of a repeat resistant uropathogen was reduced with time, or with an intervening culture without resistant uropathogens. Data that enables extension or narrowing of the empiric regimen in a university hospital ED population are not available. However, these data would substantially contribute to more efficient antibiotic treatment and prevention of antibiotic resistance.12
Objectives
The primary goal of this research was to study the distribution of uropathogens and their antibiotic resistance patterns in a university hospital population. Second, we investigated susceptibility to the empiric regimen consisting of cefuroxime and gentamicin in this population, and studied the probability of extending or narrowing of this regimen, based on previously cultured pathogens.
MATERIALS AND METHODS
Study design, setting, and patients
We conducted an observational retrospective study in the Erasmus MC. This is the largest university hospital of the Netherlands with approximately 32,000 adult ED visits per year. All urinary cultures with at least one pathogen and an available antibiogram taken from patients visiting the ED from January 1st, 2013 until December 31st, 2014 were obtained from the Department of Medical Microbiology and Infectious Disease.
Urine samples were cultured by standard microbiological culture techniques. Bacterial species were identified by Matrix Assisted Laser Desorption/Ionisation Time-of-Flight Analyzer Mass Spectrometry (MALDI-TOF MS) analysis (Microflex, Bruker Daltonics, Bremen, Germany). Susceptibility testing was performed with VITEK®2 (bioMérieux, Marcy l’Etoile, France). Antibiotic resistance was determined according to the European Committee on Antimicrobial Susceptibility Testing (EUCAST) clinical breakpoints.13 Only samples from patients 18 years or older having a UTI were included (i.e., index culture). Patients were only included once, and the first obtained sample of each patient in the abovementioned period was used. Uropathogens were considered to be identical (i.e., the same uropathogen), if the index culture and previously cultured uropathogens as well as its antibiotic susceptibility were identical.
Variables
For each patient, demographic data (e.g., age, sex, previous medical history) and data concerning their ED visit, such as history, vital parameters (e.g., blood pressure, heart rate, respiratory rate, oxygen saturation, temperature), laboratory results (e.g., C-reactive protein (CRP), leukocyte count, and presence of pyuria, defined as leukocytes in urine dipstick), results of blood cultures, previous urinary cultures acquired within 12 months prior to the ED-visit with antibiogram available, data on initiated antibiotics, and disposition were obtained from electronic patient records. In patients who were previously hospitalised in the Erasmus MC, the dates of the last admission and discharge were obtained, and time since last admission and duration of the last admission were calculated. The number of admissions in the last year was also obtained. Comorbidities considered relevant were renal transplantation, urological anomalies (e.g., recent urological interventions, neo-bladder reconstruction, urological tract anomalies), and immunocompromised status (defined as patients with congenital or acquired immunodeficiency, patients undergoing active treatment for malignancies, patients using immunosuppressive medication). Patients were grouped in ‘never hospitalised within the Erasmus MC’ (Erasmus MC-naïve), and ‘previously hospitalised in the Erasmus MC’. Previously hospitalised patients were categorised based on the time between the last admission, either > 12 months or ≥ 12 months ago. We made a subset of patients recently hospitalised (defined as < 3 months). Data on hospitalisation in other hospitals or residing in a nursing home were not available.
We combined the SWAB definition3 and the Centers for Disease Control and Prevention (CDC) definition14 to define a cUTI: an urinary culture with no more than two species of organisms identified, at least one of which is a bacterium of ≥ 103 colony forming units (in contrast to the ≥ 105 colony forming units, as defined in the CDC definition) and one of the following criteria: 1) a positive blood culture from the same moment with the same micro-organism as in the urinary culture; 2) a body temperature > 38.0 °C; 3) symptomatology of a UTI (e.g., dysuria, urinary frequency or urgency, suprapubic or costovertebral tenderness); or 4) according to the treating physician (i.e., UTI reported as (most likely) diagnosis in discharge letter). A UTI was considered to be complicated when there were signs of systemic illness. Patients met our definition of cUTI when they were fulfilled at least one of the following: being male and older than 39 years,3 having a body temperature > 38.0 °C, meeting two or more systemic inflammatory response syndrome (SIRS) criteria (of note, missing SIRS criteria were coded as negative),15 having costovertebral tenderness, being ill according to the treating physician, having a CRP > 60 mg/l,16 having a blood culture with the same pathogen as in the urine culture, having a renal transplantation in medical history, being immunocompromised, or the decision for hospitalisation by the treating physician. Cefuroxime combined with gentamicin was considered empiric therapy in the ED, and we therefore described the proportion of patients having a UTI in whom empiric therapy would have been an adequate antibiotic regimen without resistance of the causing pathogen against these agents. We also described the population of pathogens cultured with their susceptibility to different, frequently prescribed antibiotic regimens, including susceptibility to cefuroxime and gentamicin, in Erasmus MC-naïve versus previously hospitalised patients (< 12 versus ≥ 12 months ago). We compared the index culture and its susceptibility for the prescribed antibiotic regimen with previously cultured pathogens. Lastly, we compared prevalence susceptibility of uropathogens for frequently prescribed antibiotics in our population with national antibiotic susceptibility.17
Statistical analyses
We presented patient characteristics as mean and interquartile range (IQR), or as an absolute number (proportion) with percentage (%) and 95% confidence interval (95% CI). Categorical variables were compared using the Pearson chi-squared test. We performed one sample T-tests for the comparison of proportions and 95% CIs of susceptibility in our population with Dutch national susceptibility data (NethMap).17 We performed univariate and multivariate logistic regression analysis on susceptibility of the found bacteria for initiated therapy, empiric therapy and cefuroxime monotherapy over days since last admission. Other factors included in the models were sex and age. Results are presented as odds ratios (ORs) and 95% CIs. All analyses were conducted with IBM SPPS Statistics for Windows version 21 (IBM Corp., Armonk, N.Y., USA). A p-value < 0.05 was considered significant.
RESULTS
Inclusion of patients
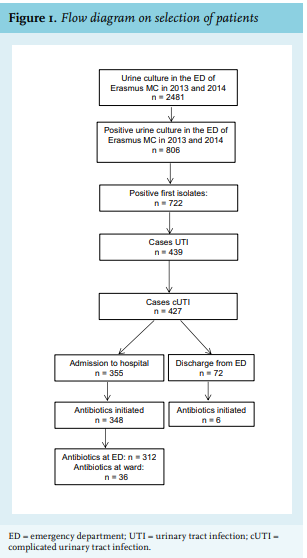
A total of 2481 urinary cultures were obtained in the ED between January 1st, 2013 and December 31st, 2014, of which 806 (32.5%) contained at least one pathogen. After selecting first isolates, 722 (89.6%) cultures of unique patients remained. Of these patients, 439 (60.8%) had a UTI according to the predefined criteria and 427 had a cUTI. A total of 355 (83.1%) patients were admitted to the hospital, and in 348 (98.0%), antibiotics were initiated. The flowchart of these results and medical decisions with respect to hospital admission and initiation of antibiotics is shown in figure 1.
Patient characteristics
Of the 427 patients with cUTI, a majority were male (223 patients, 52.2%), with a median age of 59 years. The vast majority of patients had relevant comorbidities (72.8%) and 63.2% were hospitalised the prior year. Only 12.2% of the patients were not previously admitted to Erasmus MC. Most frequently cultured pathogen was E. coli (51.3%). Other frequently cultured micro-organisms were K. pneumoniae, E. faecalis, P. mirabilis, P. aeruginosa, and S. agalactiae (Group B Streptococcus) (9.5%, 9.7%, 6.7%, 5.6% and 2.6%, respectively). Patient characteristics are shown in table 1. 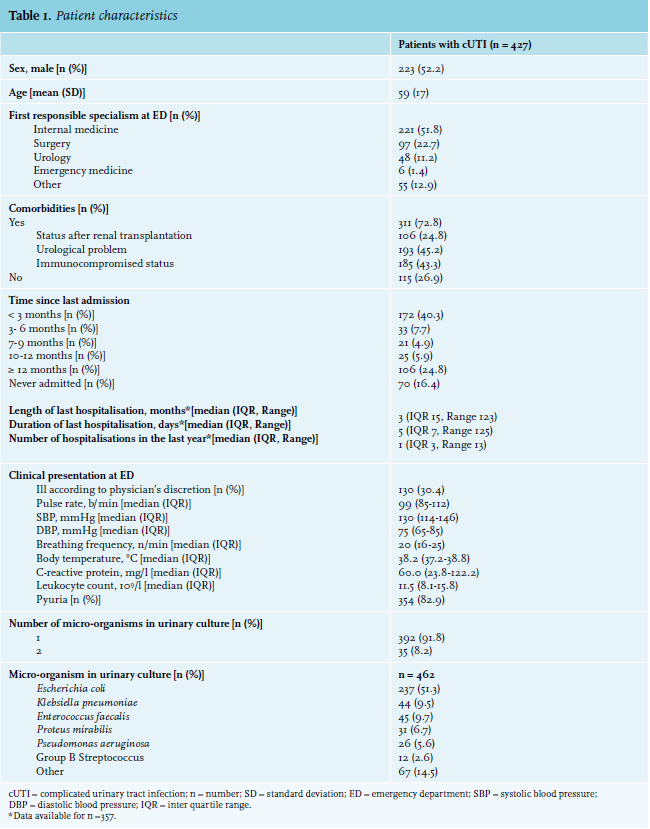
Antibiotic susceptibility
In all patients who were hospitalised after their ED visit with a cUTI, we found susceptibility to cefuroxime and/ or gentamicin in 96.2% (228/237) for E. coli, 90.9% (40/44) for K. pneumoniae, and of 100% (31/31) for P. mirabilis. These rates are comparable to NethMap-data.17 Susceptibility to meropenem was 100%, except for P. aeruginosa (susceptibility rate 92.3% (24/26)). Compared to the general resistances rates in the Netherlands, we found more resistance of E. coli and K. pneumoniae for trimethoprim-sulfamethoxazole and more resistance of E. coli and P. mirabilis for ciprofloxacin. All susceptibility patterns can be found in table 2A.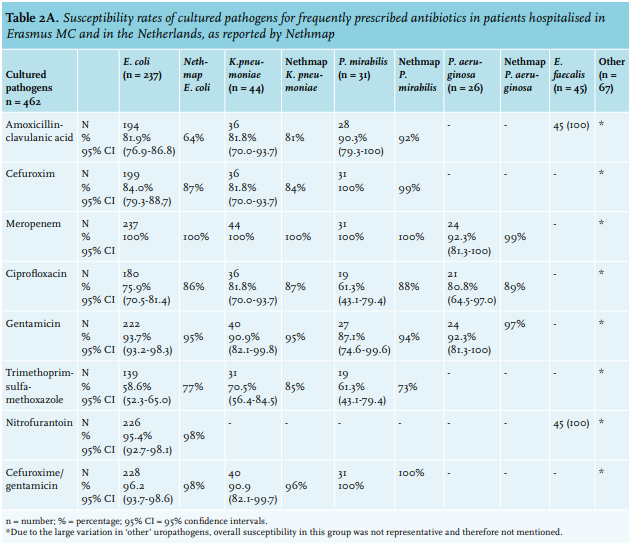
Using multivariate logistic regression, we found that a shorter time between the last admission to Erasmus MC was associated with lower susceptibility rates for initiated antibiotic therapy (OR 1.22; 95% CI 1.04, 1.43; p = 0.015). We also found that a shorter the time since the last admission was associated with lower susceptibility for cefuroxime (OR 1.31; 95% CI 1.14, 1.49; p < 0.001). We found no association between age and sex and susceptibility (OR 1.30; 95% CI 0.73, 2.31; p = 0.364, and OR 0.98; 95% CI 0.97, 1.01; p = 0.19, respectively). We also found no association between the time in days between the last admission to Erasmus MC and susceptibility for empirical therapy (i.e., cefuroxime and gentamicin) (OR 1.17; 95% CI 0.95, 1.45; p = 0.14).
We tested non-linearity by adding a quadratic term to the natural logarithm of days since the last admission to Erasmus MC. We detected no non-linearity, which implies there is no specific cut-off period for losing non-susceptible uropathogens.
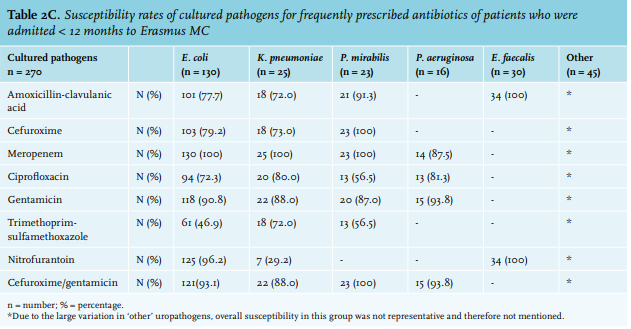
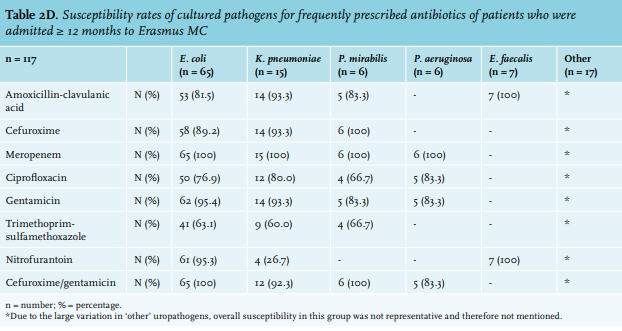
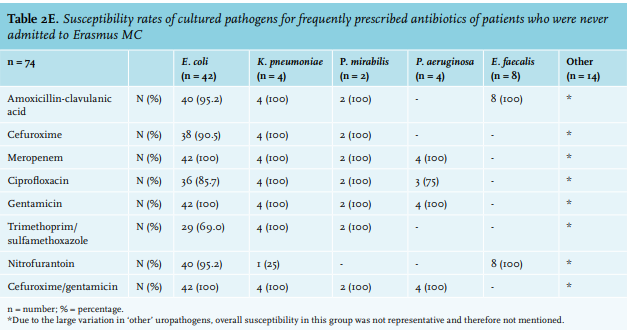
Susceptibility for amoxicillin-clavulanic acid, cefuroxime, gentamicin, trimethoprim-sulfamethoxazole, and cefuroxime/gentamicin was lowest if last admission < 3 months ago, and highest for never admitted patients (tables 2B-2E).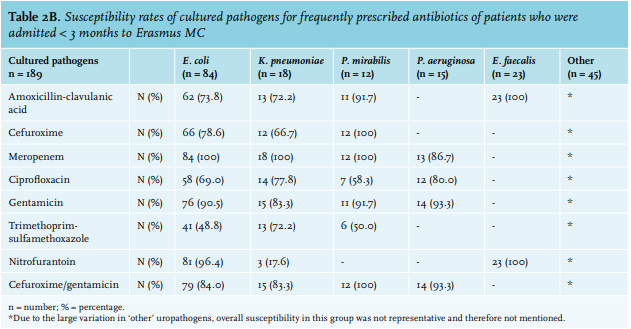
In 427 patients with a cUTI, 462 pathogens were cultured (427 single isolates, 35 double isolates). Of 185 index cultures, previous cultures were available. Of all urine cultures obtained within the last year, 56.2% (104/185) contained pathogens different from the index culture. In 71.2%, the current pathogen was susceptible for the initiated antibiotic therapy, compared to 91.4% if the pathogen matched previous cultures (p < 0.001, see table 3).
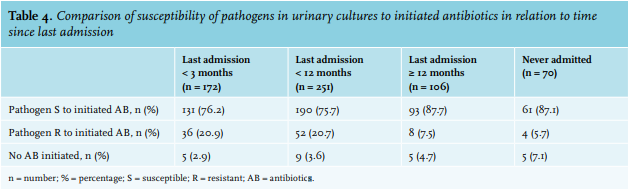
Of the 427 patients with cUTI, 61 were Erasmus MC-naïve, 251 were admitted < 12 months, and 106 were admitted ≥ 12 months ago. In patients admitted < 12 months ago, uropathogens carried higher resistance rates for the initiated treatment than those of patients who were last hospitalised ≥ 12 months ago, or were never hospitalised (24.3% vs 12.3% vs 12.9%, respectively; p = 0.002, see table 4). Majority of the patients admitted < 12 months ago were admitted in the last three months (68.9%).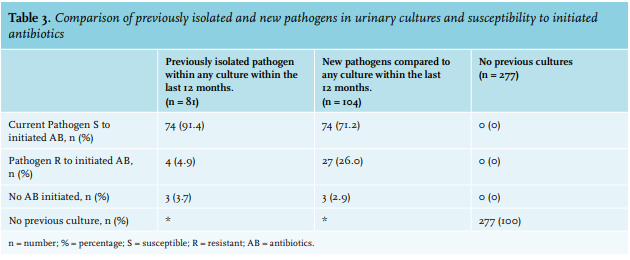
DISCUSSION
Our study shows that susceptibility rates to empirical intravenous antibiotic therapy in our cohort of patients visiting the ED of a Dutch university hospital are comparable to national epidemiological data. However, resistance to orally available antibiotics is higher for the most frequently cultured pathogens. A shorter time between presentation in the ED and the last admission was associated with lower susceptibility of uropathogens for initiated antibiotic therapy.
As in most studies, we found higher susceptibility rates for meropenem than for cefuroxime and/or gentamicin, which is aligned with NethMap 2018,17 and are most likely the result of restricted use of carbapenems, since they are considered last-resort antibiotics. In line with the principles of antimicrobial stewardship, carbapenems should continuously be prescribed with caution.18
We also found that susceptibility of prevalent uropathogens to frequently prescribed oral antibiotics was lower than nationwide susceptibility rates, especially for ciprofloxacin and trimethoprim-sulfamethoxazole. This difference is most explicit within the subgroup of patients who were admitted within one year before presentation at the ED. It is likely that this discrepancy is due to the specific patient population encountered in university hospitals. Patients who are using immunosuppressive medication or who have anatomical anomalies frequently require treatment with antibiotics and are more often admitted. These patients are not only at risk for UTIs in general, but also for UTIs with more uncommon and more resistant uropathogens.19,20 Notably, the NethMap report calculates resistance percentages for all hospitals combined and not for university hospitals separately, which probably resulted in higher susceptibility rates.
More than half of the cultured uropathogens differed from previously cultured uropathogens. This finding suggests a high prevalent heterogeneity of uropathogens in single individuals. There was significantly higher resistance for initiated antibiotics in patients who were admitted < 12 months ago, compared to patients admitted ≥ 12 months ago. This confirms the evidence that patients who are frequently admitted to the hospital carry more resistant uropathogens than patients who are less frequently or never admitted.11,21 We were not able to define a safe cut-off point, since we found a linear association over time, and the longer the time since last hospitalisation, the smaller the risk. A cross-sectional study of Teunis et al. on duration of carriership of multi drug resistant E. coli in a subset of a general adult population showed that the estimated time to lose carriership was approximately 400 days.22 In the prospective COMBAT (Carriage Of Multiresistant Bacteria After Travel) study, 633 individuals acquired multi drug resistant E. coli during travel, in whom median duration of colonization after travel was 30 days, and of whom 11.3% remained colonized 12 months after return; however, this was performed predominantly with individuals without comorbidity and infections.23 In clinical practice, the results of previously obtained cultures contribute to the decision to initiate an antibiotic regimen, but information from earlier obtained cultures should be applied with caution. Based on our data, we suggest treatment with empiric therapy, including gentamicin, in all patients – also those who were admitted recently. Antibiotic regimen should be extended and not narrowed, based on cultures obtained in the year before presentation at the ED.
In kidney transplant recipients or patients with severe pre-existent renal insufficiency (eGFR < 30 ml/min) there is continuous discussion on the safety of gentamicin. Evidence for significant nephrotoxicity after a single dose of aminoglycosides is controversial,7,24 but most physicians are cautious with prescribing aminoglycosides in patients with kidney transplants or severe renal insufficiency.21,25 However, these patients accounted for a substantial part of our study population, and for this group, monotherapy with cefuroxime or ciprofloxacin is not advisable, since susceptibility rates were below the threshold of 90%. In these selected groups another empiric regimen, like meropenem, may be justified. Especially in tertiary hospitals, where decision-making regarding the choice for antibiotic treatment in an aging, multi-morbid patient population is often complex, antimicrobial stewardship is recommended. However, we also show that guidelines on empiric therapy based on local resistance data are effective, as long as they are followed.
Due to the retrospective nature of our study we encountered several limitations. We selected patients based on positive urinary cultures and subsequently selected patients with cUTIs. In a small but substantial group, this led to misclassification of cUTI: antibiotics were initiated in only six of the 72 patients who met our criteria for cUTI and who were discharged from the ED. Patients with cUTI without positive urinary cultures, for example, due to pre-treatment with antibiotics or due to a negative urinalysis and no subsequent culture, were not selected. This might have led to a selection bias. However, our data (i.e., the cultured uropathogens and their antibiotic susceptibility) were selected are used in the national NethMap data. We also have no information on antibiotic treatment of patients in general practice or in other hospitals, and if antibiotics would have been used, this could potentially have caused an increase in resistance in our population.
Also, important differences between our data and NethMap 2018 results are seen in the susceptibility rates of E. coli and K. pneumoniae for amoxicillinclavulanic acid. This is a result of a new test panel for Gram-negative bacteria, resulting in higher minimal inhibitory concentrations for amoxicillin-clavulanic acid and higher resistance levels from 2016 onwards. For our data, susceptibility rates from the period 2013-2014 are applicable. Therefore, we compared our data with NethMap reports for this period and our resistance percentages for amoxicillin-clavulanic acid are comparable.17
In conclusion, the distribution and antibiotic susceptibility for intravenous antibiotics of uropathogens in a Dutch university hospital is comparable with overall distribution in the Netherlands. Cefuroxime in combination with gentamicin is therefore an adequate antibiotic regimen for cUTI, and we recommend treating patients accordingly. Extension of the chosen regimen based on earlier cultured pathogens is advised, and narrowing of the antibiotic regimen strongly discouraged, especially the omission of gentamicin. In a strictly selected population (e.g., recently admitted renal transplant recipients, pre-existing severe kidney insufficiency), prescription of meropenem as an alternative empiric therapy could be considered.
REFERENCES