KEYWORDS
Chronic hepatitis; hepatitis B virus; retrieval; REACH
INTRODUCTION
In the Netherlands, approximately 200 people die annually from the consequences of hepatitis B virus infection.1 With an estimated prevalence of 0.34% for chronic hepatitis B (CHB) in the Netherlands, there are roughly 49,000 patients who are chronically infected.2 The current availability of new and effective treatment modalities for CHB leads to more patients being eligible for treatment, which reduces liver-related morbidity and mortality. However, many patients who were once diagnosed with CHB are no longer in care and are therefore unaware of these new treatments.3 Several regional CHB retrieval projects described a loss to follow-up (LFU) rate up to 65%.4-6 For this reason, in 2014, the Dutch National Institute for Public Health and the Environment (RIVM) requested that the various parties involved retrieve and evaluate patients once diagnosed with CHB and offer them treatment.7 This aligns with the goals of the Dutch national plan on viral hepatitis and the World Health Organization (WHO) targets to prevent or even eliminate further distribution and burden of disease as a consequence of viral hepatitis.8,9
In September 2016, the University Medical Centre Utrecht (UMCU) partnered with hepatitis treatment centres and the Public Health Services (GGD) in the Utrecht region and initiated the REACH (REtrieval And Cure of Chronic Hepatitis C) project. This project entailed retrieval of patients with chronic hepatitis C who were no longer in care to provide them with a (serologic) evaluation and an appropriate treatment plan.10 Following the REACH project, the GGD started with the retrieval of patients who were previously diagnosed with CHB but were LFU. In contrast to patients with hepatitis C, not every patient with hepatitis B qualifies for treatment. This made the retrieval project for these patients less applicable. As the decision to begin treatment is dependent on multiple parameters such as the hepatitis B virus (HBV) viral load, liver fibrosis stage, and degree of inflammation, and adequate care for a patient with CHB includes not only treatment in a hepatitis treatment centre, but also periodic follow-up by the general practitioner (GP).11,12 This article describes the results of this hepatitis B retrieval project in the Utrecht region in the Netherlands which constitutes the largest CHB retrieval project to date.
MATERIALS AND METHODS 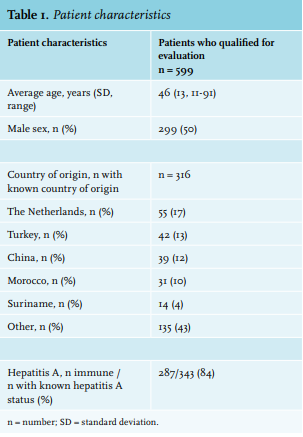
The four hospitals in the Utrecht region (University Medical Centre Utrecht (in collaboration with Gelderse Vallei Hospital), Diakonessenhuis, St. Antonius Hospital, and Meander Medical Centre; all designated hepatitis treatment centres) participated in this project. For each hospital, a list was compiled of all patients with a positive HBsAg result in the period from 2001 to 2015. The chosen 15-year time period was based on the care provider’s duty of care, which includes keeping patient medical records for 15 years after the end of treatment and informing the patient when new treatments become available. In accordance with this duty of care legislation and the Dutch Medical Treatment Act (WGBO), the medical microbiologists directly involved in the treatment were allowed to exchange information with the patient’s GP.7 Electronic medical records were reviewed to determine whether a patient qualified for (serologic) evaluation by the GP. Patients qualified if they (1) had a chronic hepatitis B infection (i.e., the last available HBsAg was positive and measured between January 1st, 2001 and December 31st, 2015); (2) were not currently undergoing treatment or being followed-up by a medical specialist (i.e., no appointment was scheduled after January 1st, 2016); (3) lived in the Utrecht region; and (4) the name and address of their GP was available. Other relevant information on demographic, clinical, and laboratory data, such as country of origin and hepatitis A status, were extracted from the electronic medical records. Of the patients who qualified based on the predefined inclusion criteria, the GP was requested in January 2018 in writing, to evaluate the patient in agreement with the ‘guideline on viral hepatitis’ from the Dutch College of General Practitioners (NHG) and to refer the patient accordingly if necessary (i.e., in case of raised alanine aminotransferase (ALT) levels, a positive HBeAg or an HBV-DNA ≥ 2000 IU/mL).11 Moreover, GPs were asked to fill out a questionnaire with questions on patient characteristics (see table 1) and hepatitis A status, and to indicate reasons for not being able to perform a re-evaluation. If a patient was no longer registered at the GP’s practice, the GP was asked to contact the investigator and, if known, provide the name of the current GP. Both data from the questionnaires and information from contact with the GPs via telephone or email were collected. The GPs were asked to evaluate the patient and/or return the questionnaire within six months. Thereafter, it was ascertained whether the patients who were referred by the GP did indeed visit the hospital.
The execuon of this retrieval project took approximately 350 hours. The majority of time was spent on the review of the patients’ electronic medical records. The Medical Research Ethics Committee (METC) of the University Medical Centre Utrecht (METC code 041, file number 12-409) declared that the Dutch Medical Research Involving Human Subjects Act (WMO) did not apply to this project and had no objection to the execution of this study.
Statistical analysis
Continuous data are reported as means with standard deviation (SD) and discrete variables in absolute and relative frequencies. Descriptive statistics were generated with IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp.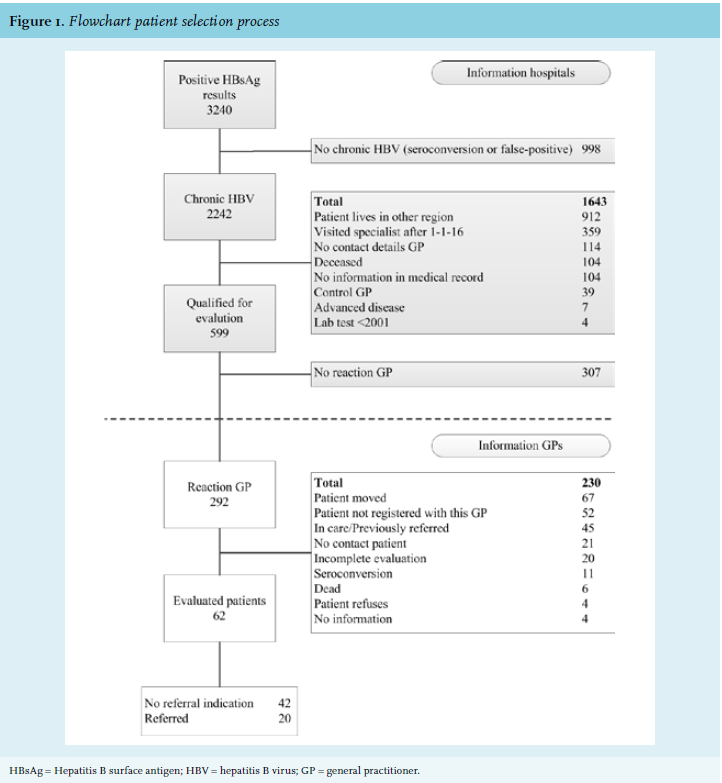
RESULTS
Initially, 3,240 unique positive HBsAg test results between the years 2001 and 2015 were extracted from the laboratory records of the four participating hospitals (figure 1). After review of the patients’ medical records, 2,641 patients were not suited for retrieval: 998 patients (38%) did not have a chronic hepatitis B infection (e.g., seroconversion or false positive), 912 patients (35%) never lived in or no longer live in the Utrecht region, and 359 patients (14%) had visited a specialist for their CHB after January 1st, 2016 and were therefore not considered to be LFU.
A total of 599 evaluation requests and questionnaires were sent to GPs and 14 letters were resent after having received updated contact information of the GP. The demographic and clinical characteristics for the 599 patients who qualified for evaluation are summarized in table 1. The patients had an average age of 46 years (± 13 SD) and 50% were male. The country of origin was known in 53% (n = 316) and this group predominantly consisted of Dutch (17%, n = 55), Turkish (13%, n = 42), and Chinese (12%, n = 39) patients. The hepatitis A status was determined in 343 patients (57%) and 287 (84%) of those were found immune for this viral infection.
The GP response rate was 49% (n = 292) and the replies consisted of 147 filled out questionnaires and 145 emails and phone calls. Of those, 79% (n = 230) could not be evaluated, mainly because the patient had relocated (29%, n = 67) or was no longer registered with the GP (23%, n = 52), and follow-up information was unavailable. The remaining part (21%, n = 62) was evaluated by the GPs.
Of the evaluated patients, 42 patients (68%) did not have an indication to be referred to a hospital according to the NHG guideline and 20 patients (32%) were referred. Of the referred patients, 14 had visited a hepatitis treatment centre, an appointment was planned for two patients, and four patients had made an appointment but did not attend. Of the 14 patients who have already visited the outpatient clinic, one started treatment. For the other 13 patients, at the writing of this manuscript, there is either no indication to start treatment (n = 10) or they are still awaiting the results of additional laboratory testing (n = 3).
DISCUSSION
This study aimed to trace all LFU CHB patients in the Utrecht region in the Netherlands by means of screening past positive HBsAg results. At the end of the study, 10% of all LFU CHB patients eligible for retrieval had been evaluated by their GP and 3% were referred to a hepatitis treatment centre. The GPs were willing to participate in CHB care and retrieval as is reflected by the response rate of 49%. To our knowledge, this is the largest CHB retrieval project that has been conducted to date. Other Dutch CHB retrieval projects previously achieved response or evaluation rates of 44-70% but these cannot be directly compared with the current study due to different methods and LFU definitions that were used in each project.4-6 In the study of Beekmans et al., 44% of the invited patients were finally evaluated at the hospital. However, deceased patients and patients with an unknown GP had been completely excluded from the analysis which could partly explain the higher success rate.6 The study of Spruijt et al. reported a GP response rate of 70% but this involved both hepatitis B and C patients and also included false-positive results.4 Beekmans et al. described that three CHB patients had an indication for antiviral therapy but not how many actually started treatment. One patient initiated treatment in the current study but this number may still increase since three patients were still awaiting the results of additional investigations.6
A total of 2,242 CHB patients were identified in the Utrecht province after evaluation of a 15-year time period. However, almost double the number of CHB-infected patients would be expected based on the prevalence of 0.34% and the Utrecht population size of almost 1.3 million inhabitants. Our numbers align with the nationwide notification data on CHB from the RIVM who also report a ~ 50% diagnosis rate when compared to the total population size estimates.13 All though differences in our study population size may partly be explained by local CHB prevalence differences and the exclusion of GP laboratory records from this project, it also suggests that a substantial number of CHB infected remain undiagnosed.
Because this project focused on the Utrecht region, 912 (41%) of the identified CHB patients who currently reside outside of Utrecht were excluded. This high number of non-Utrecht residents is probably inherent to the large total adherence area of the four hospitals combined. Also, GPs described asylum seekers as a very dynamic population as they were often relocated after initial testing for CHB had been performed by a nearby asylum seekers’ centre. Retrieval projects specifically targeting this risk group would therefore be a worthwhile future endeavour in our opinion. These could complement the Health Council’s (HC’s) recommendations to screen all asylum seekers from endemic countries for CHB.14 First-generation migrants are also included in the HC’s advice as they are, by far, the largest subgroup affected by CHB in the Netherlands.2 More specifically, Turkey, Somalia, and China are the main countries of origin in Dutch CHB-infected first-generation migrants.15 This is also reflected in our population eligible for retrieval which included 83% of non-Dutch individuals and Turkey and China as the largest migrant groups. Only the Somalis seemed underrepresented in our study population compared to the nationwide estimates, however this could be due to the high proportion of unknown countries of origin in our group.
This retrieval had a positive effect on the renewed linkage to care of CHB patients and possible treatment initiation among GPs in the Utrecht region. In addition, a reinstituted periodic follow-up of CHB patients without referral indication is also considered a positive outcome of this retrieval effort. Through this project, the GPs have become reacquainted with the 2016 updated NHG guideline on viral hepatitis which now recommends indefinite periodic control of ALT and HBsAg in “inactive CHB carriers”.11 We anticipate that an increased number of GPs will resume this regular follow-up of CHB patients after this reintroduction.
Another positive effect that was expected from this project is the raised awareness of CHB among GPs which may result in evaluation of other LFU CHB patients and also increased screening practices. Indeed, preliminary notification data of the GGD suggest enhanced screening efforts: the number of reported CHB in the six months after this project had increased to 44 in comparison with 32 notifications during the same period in 2017. However, subsequent studies may need to confirm this assumption by following-up with the participating GPs over a longer period of time. A final positive side effect of this project was the multidisciplinary collaboration for this project, leading to a reinforcement of the regional healthcare network.
The main drawback of this project was that the GPs’ laboratory records at the medical diagnostic centre Saltro, could not be included. Therefore, the LFU CHB patients who had never been referred to a hepatitis treatment centre could not be retrieved. Future retrieval initiatives should focus on tracing these specific LFU CHB patients and bringing them back into care.
For the benefit of future HBV retrieval efforts, the key lessons learned were distilled from this project. First, written evaluation invitations should be short and straightforward and additional information for research purposes is preferably requested separately in order to optimize the evaluation response rates. For further time saving purposes, the NHG referral guidelines may best be summarized in the invitation letter. Second, it could be beneficial to offer the GP remote (tele-) supervision from a hepatitis specialist since they often perceive hepatitis B serology as difficult to interpret and only have a few chronic HBV patients in their practice. Third, in order to optimize the GPs’ response rate, it is essential to learn more about the GPs’ perceived barriers and facilitators to participation in HBV retrieval projects.
CONCLUSION
Lost to follow-up CHB patients can be traced through screening of past positive HBsAg tests and GPs are willing to participate in the retrieval of CHB patients. This may contribute to the reduction of the CHB related burden of disease.
DECLARATIONS
Acknowledgements
The authors wish to thank L. Huyveneers for her help with reviewing the electronic medical records. The secretarial work from the Department for Infectious Disease Control of the Public Health Services (GGD) Utrecht is also greatly appreciated.
**REACH working group
A.I.M. Hoepelman MD PhD and G.J. Boland MD PhD of the UMC Utrecht in Utrecht, B.J.M. Vlaminckx MD PhD and P.H.G.M Stadhouders MD of the St. Antonius Hospital in Nieuwegein, S.F.T. Thijsen MD PhD and M.A.M.T. Verhagen MD PhD of the Diakonessenhuis in Utrecht, P.W. Friederich MD PhD and A.J.L. Weersink MD PhD of the Meander Medical Centre in Amersfoort.
Conflict of interest statement
Dr. Arends reports fees from Abbvie, BMS, Gilead, Janssen, MSD and ViiV and research grants from Abbvie and BMS, outside the submitted work, all paid to his institution. Dr. Boland is Chairman of the Hepatitis Information Foundation, which is supported by AbbVie, Gilead, BMS and GlaxoSmith Kline. Fees go to the department of Medical Microbiology, UMC Utrecht. Dr. Hoepelman reports personal fees from Abbvie, BMS, Gilead and Janssen. All other authors declare that they have no competing interests with respect to the presented work.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
REFERENCES