DIAGNOSIS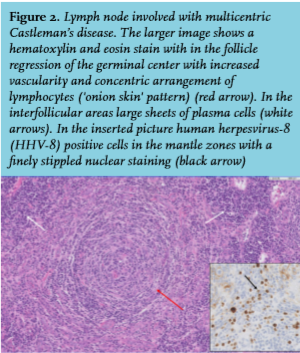
The FDG PET/CT scan shows extensive lymphadenopathy and splenomegaly suggestive for multicentric Castleman’s disease (MCD), although malignant lymphoma, opportunistic infections and sarcoidosis cannot be excluded. Histology and immunohistochemistry of an excised axillary lymph node confirmed the diagnosis of MCD and immunostaining for human herpesvirus-8 (HHV-8) on biopsy was positive (figure 2).
MCD is a recurring and remitting lymphoproliferative disorder with an incidence in HIV patients of around 8.3 per 10,000 patient-years, in which it is associated with HHV-8.1 The pathogenesis is related to infection of HHV-8 in immunoblasts and the production of viral interleukin-6 (IL6), but the exact mechanism is unknown. CD4 counts and viral load at presentation can vary and are not associated with the risk of developing MCD. Patients typically present with fever and lymphadenopathy. Splenomegaly, hepatomegaly and fluid retention are also common findings and concomitant Kaposi sarcoma is found in approximately 70% of the patients.2 Histologically, pathological variants of lymph node biopsies can be divided into three categories: The plasma cell variant and the mixed variant each represent approximately half of cases, the hyaline vascular variant represents 4%. HHV-8 testing on biopsy or serum is positive in 98% of cases associated with HIV. Diagnosis is made when clinical criteria as described by the French Agence Nationale de Recherche sur le SIDA 117 CastlemaB trial group are met, in combination with histological findings.1,2,3
Evidence on the treatment for MCD is of low quality, current expert opinion is to treat with rituximab. Multiple studies have combined rituximab with antiviral therapy or with chemotherapy, but evidence is of low quality due to small study populations. Anti-IL6(R) therapy shows promise as a second line regimen, but is still under investigation. Antiretroviral therapy (ART) needs to be initiated in newly diagnosed HIV patients and optimized in existing ones already on ART. However, MCD can also be provoked by a rise in CD4 count in the context of an immune reconstitution inflammatory syndrome, as could have been the case in our patient.2 All-cause mortality for HIV patients with MCD is high, around 25% with a median follow-up of 27 months.1,3 Imaging is not always necessary for diagnosis but an FDG PET/CT-scan can assist in distinguishing from concurrent conditions, can aid in choosing a lymph node to excise and can confirm complete remission after initial treatment.4 Our patient was treated with rituximab and valganciclovir for four weeks and showed complete remission on a follow-up FDG PET/CT-scan three months later.
ACKNOWLEDGEMENTS
We thank dr. L.B. Meijer-Jorna for disclosure of imaging of histology and immunohistochemistry.
REFERENCES