KEYWORDS
Acute CMV infection, cytomegalovirus, portal vein thrombosis, pulmonary embolism, venous thromboembolism
INTRODUCTION
Approximately 65% of the general population will become infected with the cytomegalovirus (CMV), in 50% during adulthood. The manifestation of CMV infection varies from asymptomatic or mild mononucleosis-like syndrome to a severe, disseminated infection in immunocompromised patients.1 It is not generally known that acute CMV infection is associated with arterial and venous thromboembolism (VTE).
CASE PRESENTATIONS
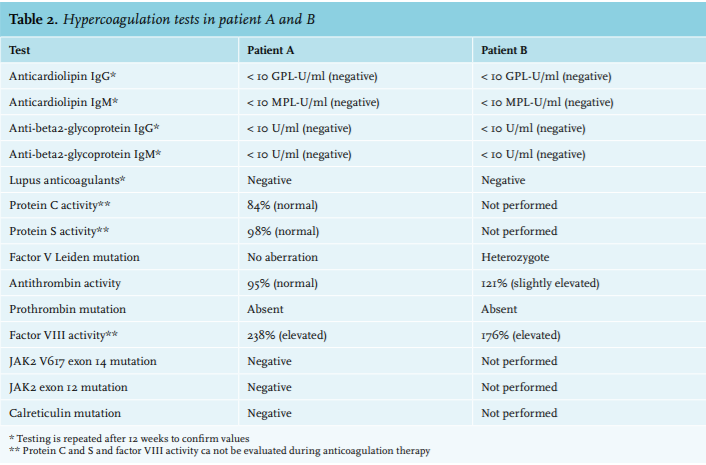
Patient A, a 66-year-old man, presented to the emergency department (ED) with abdominal pain. In the last month he had been investigated elsewhere because of fever, anorexia, fatigue and mildly elevated liver enzymes. Because of hypotension, tachypnoea and lactic acidosis upon ED presentation, an abdominal computed tomography scan with intravenous contrast was performed that showed intestinal ischaemia due to extensive portal vein thrombosis. Anticoagulant therapy was started and partial resection of the small intestine was performed, followed by a long and complicated stay in the intensive care department. The portal vein thrombosis was regarded as unprovoked and both the family history and thrombophilia testing were negative. Eventually, the results of the serological tests (which were requested before the time of presentation at the emergency department) became available and showed evidence for acute CMV infection (table 1). Apart from the acute CMV infection, he had no thrombophilic risk factors. Anticoagulant therapy was stopped after 15 months during follow-up in the outpatient clinic and he is currently rehabilitating in a nursing home.
Patient B, a 60-year-old woman, presented to the ED with chest pain, fever and dyspnoea. The initial chest X-ray and electrocardiogram showed no explanation for her symptoms. Three weeks earlier, she had visited our outpatient clinic with fatigue, fever and muscle pain. CMV testing at that time revealed an acute CMV infection as an explanation for her symptoms. Additionally, the family history revealed that her mother had died postpartum of venous thromboembolism. A CT scan was performed and showed massive pulmonary embolism together with a pulmonary infarction. She became haemodynamically unstable and was transferred to the intensive care unit to initiate thrombolytic therapy, followed by treatment with anticoagulant therapy. Hypercoagulability testing revealed heterozygosity for the factor V Leiden mutation (table 2). Patient B is being treated with lifetime anticoagulation (direct-acting oral anticoagulants) because of the positive family history, the severity of the thrombotic event and the heterozygosity for the factor V Leiden mutation. She was discharged home after a short hospitalisation and has recovered completely.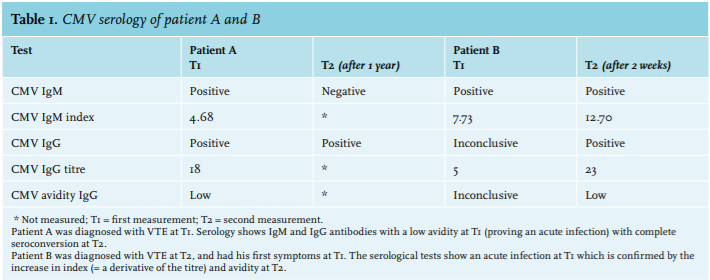
DISCUSSION
Although more than 100 patients with both venous and arterial CMV-associated thromboembolism are reported in the current literature, this association is not generally known. Based on the results of several studies, which are discussed below, it seems that CMV forms a risk factor for arterial and venous thromboembolism. However, this is not mentioned in the current Dutch guidelines. In our two immunocompetent patients we performed additional tests for hypercoagulability because of the extensive thrombosis and severity of symptoms (table 1). Serological tests for CMV were performed in both patients because they initially presented with mononucleosis-like syndrome (table 2).
Epidemiology
In a large meta-analysis reporting 97 patients, thrombosis incidence of 6.4% is reported in hospitalised adult patients with an acute CMV infection. Conversely, an acute CMV infection is detectable in 2-9% of the hospitalised patients with VTE, versus 1.6% CMV infections in the control group without VTE. Although patients are usually exposed to CMV during childhood and adolescence, CMV-associated thrombosis occurs mainly in adults, as in our patients. In this meta-analysis reporting on 97 patients with CMV-associated thrombosis, the mean age was 40 years (25-55 years), the most common sites were deep vein, pulmonary or splanchnic vein thrombosis and immunocompetent patients more often had a genetic or acquired predisposing thrombophilic factor relative to immunocompromised patients.2 CMV may be the last trigger needed to provoke thrombosis in these patients. In other studies, CMV was the only detectable risk factor for thrombosis in immunocompetent patients.3
Pathogenesis
Viral hepatitis can induce a procoagulant state due to inflammation. However, CMV is more strongly associated with venous thromboembolism than other herpes viruses that can lead to hepatitis, such as the Epstein-Barr virus for instance.4 CMV seems to interfere directly with haemostasis and several pathogenetic mechanisms have been described explaining its role in thrombosis (figure 1). CMV activates in vitro factor X and stimulates the production of factor VIII and von Willebrand factor. CMV binds to platelets via Toll Like Receptor 2, thereby presenting the adhesion molecule P selectin on the cell surface. In addition, CMV causes systemic endotheliitis at various sites in the body, leading to expression of tissue factor. These three mechanisms result in platelet and leukocyte aggregation, adhesion and thrombin formation. In vivo, a transient increase in antiphospholipid antibodies can be observed. Also, decreased protein C activation has been described.5-8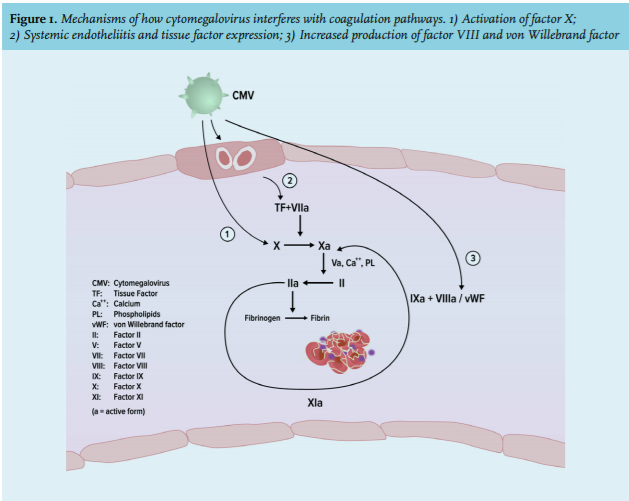
Implications for clinical practice
The Dutch national guideline ‘Antithrombotic therapy’, published in 2016, differentiates for treatment in patients with provoked or unprovoked (idiopathic) venous thromboembolism.9 CMV has specific thrombogenic characteristics and appears to be a trigger for thrombosis in patients, either in the presence or absence of other predisposing factors for thrombophilia. However, CMV is not recognised as a risk factor for thrombosis. Therefore, we advocate to perform serological testing if patients present with thrombosis and mononucleosislike syndrome. We recommend to prospectively follow this patient group in order to determine predisposing thrombophilic factors, the relative risk of CMV and thrombosis relapse risk. The estimated relative risk can be evaluated in order to determine the extent of secondary prophylaxis.
CONCLUSION
Acute CMV infection is a transient risk factor for both arterial and venous thromboembolism and can occur in immunocompetent patients in the absence of other thrombophilic factors. Based on the literature, thrombosis appears to be an underestimated complication of CMV infection. Recognition of symptoms leads to early diagnosis and treatment of complications. More research is needed to determine the relative risk of CMV as a provoking factor for thrombosis, the duration of treatment and the recurrence rate.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES