KEYWORDS
Helicobacter pylori, resistance, antibiotic stewardship, treatment.
INTRODUCTION
Helicobacter pylori is a curved, sometimes spiral, Gram-negative rod-shaped bacterium which has its niche in the gastric epithelium. Because of the production of urease and the presence of flagella, H. pylori is able to survive in this highly acidic environment. Robin Warren and Barry Marshall first isolated H. pylori in Australia in 1982. In 1985, Marshall fulfilled the postulates of Koch by infecting himself with the bacterium and in 2005 he (along with Warren) received the Nobel Prize for Medicine for demonstrating the causal link between H. pylori and peptic ulcers. In addition, H. pylori has been associated with dyspepsia and gastric cancer as well as with a number of other diseases including idiopathic thrombocytopenic purpura and iron deficiency anaemia.1 Approximately 50% of the world population is infected with H. pylori, but there is a large geographic variation. In the majority of people the infection is asymptomatic. In northern Europe and North America the average prevalence of ‘carriership’ (or asymptomatic infection) is approximately 30%, while in low-income countries this percentage may exceed 70%.2 The prevalence of H. pylori has shown a decline in developed countries over time. However, given its widespread dissemination and its potential to cause disease, recent observations that antimicrobial resistance of H. pylori is rapidly increasing may – eventually – have substantial effects on human health.3-5 It is known that the antibiotic resistance of H. pylori varies by region, for example in the UK the resistance to clarithromycin is reported to be < 10%, while in Turkey it is > 40%.2 Already as a result, failure of standard triple therapy with high-dose proton pump inhibition, amoxicillin and clarithromycin is increasing.2 Many other treatment combinations have been investigated, but trials and cohort studies showed inconsistent or incomparable results.6
Several barriers hinder the optimisation of targeted antimicrobial treatment based on susceptibility patterns, which is usual for other pathogens. An invasive endoscopic procedure including gastric and/or duodenal biopsies is needed for adequate samples for cultivation of H. pylori. Due to the fastidious nature of H. pylori these biopsies need to arrive at the laboratory within hours. Furthermore, H. pylori grows slowly and requires specific culture conditions such as an optimal medium, correct temperature and pH, as well as a microaerophilic atmosphere (i.e. lower amounts of oxygen: 5-10%). If the laboratory is capable of assessment of susceptibility patterns, agents tested usually include ampicillin (amoxicillin), clarithromycin, levofloxacin, metronidazole, rifampicin, and tetracycline.7 The presence of H. pylori can also easily and reliably be detected with cheaper, non-invasive techniques, e.g. faecal antigen tests. These are effective in settings of low prevalence of resistance.8,9 However, the use of non-invasive techniques for H. pylori detection, which do not deliver information about susceptibility patterns, will contribute to a further increase in resistance and treatment failure rates in settings with a higher a priori risk for H. pylori resistance. Hence, internationally, the treatment paradigm is now shifting towards individualised medicine.4
In the Netherlands, only a few laboratories routinely conduct resistance testing of H. pylori, and resistance data for H. pylori are not reported in the Dutch annual national resistance report (Nethmap10). At present, a lack of data precludes sufficient insight into the epidemiology of antimicrobial resistance of H. pylori in the Netherlands. Based on description of loco-regional resistance data we address the increasingly complex issue of optimising antimicrobial treatment of H. pylori infection in the Netherlands.
METHODS
Study population
In the Leiden University Medical Center biopsies for H. pylori culture are routinely performed when there is a suspicion of H. pylori infection in the anamnesis or when performing the gastroscopy. Two biopsies in the antrum and two biopsies in the corpus are sent in for culture. Culture and susceptibility results of all first H. pylori isolates of adults (> 18 years) from January 2006 to December 2015, were obtained from the database of the Department of Medical Microbiology. In addition, the surname of the patient was retrieved to discriminate between patients from autochthonous or foreign descent. Since no intervention was performed and data were anonymised prior to the final analysis, it was not necessary to obtain informed consent.
Microbiology methods
All gastric or duodenal biopsies arrived at the laboratory within several hours. Biopsies arrived in tubes with 2 ml of physiological salt 0.85% (Media Products, Groningen, the Netherlands). Cultures were incubated in microaerophilic conditions at 35°C on nonselective Columbia agar with 5% sheep blood and selective Pylori agar (bioMerieux Benelux B.V., Boxtel, the Netherlands). Campylobacter jejuni ATCC 29428 was used as a growth control and cultures were evaluated on days 3-5 and day 7 (figure 1). In case of a positive culture, further determination was performed by Gram stain and oxidase, catalase and urea tests.
Susceptibilities were determined for ampicillin, clarithromycin, levofloxacin, metronidazole, rifampicin, and tetracycline. A McFarland 3 suspension was incubated microaerophilically on Brain Heart Infusion agar (Media Products, Groningen, the Netherlands) at 35°C for 3-5 days. The minimum inhibitory concentration values, i.e. the lowest concentration of an antibiotic that prevents visible growth of a bacterium, were determined by Etest (AB Biodisk, Solna, Sweden) and categorised into sensitive (S), intermediate (I) or resistant (R) for the respective antibiotic based on the ‘European Committee on Antimicrobial Susceptibility Testing’ breakpoint tables (figure 2).6
Statistical analyses
Resistance rates for antimicrobial agents commonly used to treat H. pylori infection were compared by Chi-square tests between the periods 2006-2010 and 2011-2015. Data are presented as numbers and percentages for each antibiotic separately. To estimate influence of selection bias, in particular by receiving an indication for gastric endoscopy due to failed treatment courses for H. pylori, a random sample of approximately 5% was drawn from the original dataset to verify pre-treatment. Effect modification was verified by adding an interaction term to the model. The IBM SPSS statistical software package (version 23) was used to perform all calculations.
RESULTS
In the period from 2006-2015, H. pylori strains were isolated from a cohort of 707 adult patients. The number of isolates per year varied from 50 to 94, but did not show a rising trend over the years (linear-by-linear association test p = 0.46). The mean age of the patient at the moment of biopsy was 55 years (SD 15 years), approximately half were female (n = 369, 52.2%). The main reason for gastroscopy was dyspepsia (n = 197, 27.9%), pain in the epigastric region (n = 59, 8.3%), dysphagia (n = 46, 6.5%) or other stomach complaints (n = 69, 9.8%). Almost 12% of the gastroscopic procedures were performed to assess the aetiology of gastrointestinal bleeding (n = 44, 6.8%) or to assess the presence of varices (n=35, 5.0%). Gastroscopies were also performed in the work-up of analyses of anaemia (n = 104, 14.7%) or weight loss (n = 51, 7.2%). Only in 19 patients was the determination of H. pylori resistance the indication for gastroscopy (2.7%). The indication for gastroscopy was assessed as ‘other’ in 43 cases (6.0%) and could not be retrieved in 40 cases (5.7%). The percentage of successful determination of the antibiotic resistance percentage was about 90%. The proportion of isolates from Dutch vs. other ethnic backgrounds was stable over the years (mean 39%, range 29-48%).
For clarithromycin an increase in resistance was observed from 9.8% to 18.1% (p = 0.002) in the periods from 2006-2010 and 2011-2015, respectively (table 1). Resistance between these periods also increased for ampicillin from 6.3% to 10.0% (p = 0.37), and metronidazole from 20.7% to 23.2% (p = 0.42). In the case of tetracycline, resistance remained low at 3.2% and 2.3%, respectively. For levofloxacin, resistance was only assessed from 2013 onwards. There was no effect modification by ethnic background of the increase in resistance of H. pylori (p-value for interaction > 0.10). In our sample of pre-treatment verification, pre-treatment of H. pylori was only documented in one of 45 patients (2%).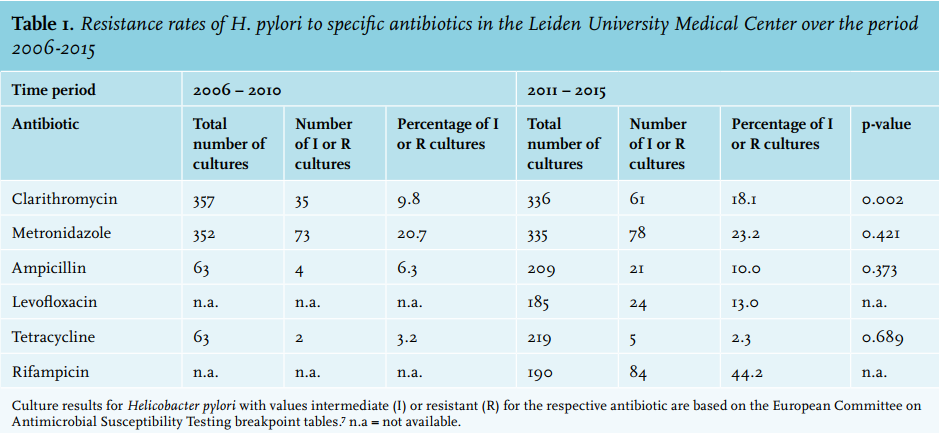
DISCUSSION
We found an increase in the average antimicrobial resistance rates of H. pylori, in particular for clarithromycin, over the last ten years. This finding does not appear to be mitigated by an increase in the proportion of non-autochthonous patients or selection of pre-treated patients. However, it cannot be completely excluded that in the general population or, for example, in a different geographic location in the Netherlands, resistance rates are lower and/or stable.11 It is expected that the effectiveness of triple therapy will decrease as a result of increasing clarithromycin and amoxicillin resistance.2 When clarithromycin resistance is present, the chances of successful treatment decrease from 90% to 44%.6 With increasing resistance, the standard regimen might actually be monotherapy with either amoxicillin or clarithromycin. This creates a negative spiral, which increases the resistance of H. pylori for both these drugs.
Future directions: choice of antimicrobials and duration of treatment
In the Netherlands, the standard policy according to the general practitioner guideline is triple therapy: proton pump inhibition, amoxicillin (2 dd 1000 mg) and clarithromycin (2 dd 500 mg) each orally for 7 days.8,9 If therapy is not successful, the current Dutch general practitioner guidelines recommend a second course of proton pump inhibition, amoxicillin (2 dd 1000 mg) and metronidazole (2 dd 500 mg) for 7 days without performance of any further diagnostic tests.8,9
In a recently published network meta-analysis different therapies for H. pylori were compared with regard to efficacy and side effects.6 A network meta-analysis pools studies in order to compare treatments which have not previously been directly compared with each other. In the current network meta-analysis 14 therapies in 143 studies were compared and ranked in terms of effectiveness (n = 32,056 patients) and adverse effects profile (n = 22,180 patients). The standard triple therapy showed to be the second least effective therapy; only a 7-day regimen based on levofloxacin performed worse. Furthermore, the analyses indicated that a longer duration of therapy was more effective, but also accompanied by more side effects. A major drawback of this study is that local resistance figures were not taken into account.4
Recently a consensus statement, based on the opinions of experts in the field, recommended first-line therapy with clarithromycin and either amoxicillin or metronidazole in regions where there is low probability (< 15%) of resistance for clarithromycin.3 In regions with high resistance rates (> 15%) against clarithromycin, quadruple therapy is advised: non-bismuth based (amoxicillin, metronidazole and clarithromycin) or bismuth based (bismuth, metronidazole, tetracycline).3 Noteworthy, in the Netherlands, bismuth is still hard to obtain. Another option suggested in the consensus statement is a levofloxacin-containing triple therapy. The consensus additionally recommended to extend the treatment duration of H. pylori to 14 days.3
CONCLUSION
Approximately 50% of the worldwide population are H. pylori carriers. H. pylori can cause dyspepsia, ulcers and gastric cancer. Our regional data suggest that H. pylori resistance is an increasing problem in the Netherlands. Based on these resistance data, the recommended standard 7-day triple therapy with high-dose proton pump inhibition, amoxicillin and clarithromycin is not always the best choice. Over time, resistance may further develop as a major cause of therapy failure. Therefore local resistance data should be taken into account when deciding about the optimal diagnostic and therapeutic strategy. In case of treatment failure, it should be strongly considered to refer a patient for endoscopy, biopsy and culture. When a second treatment based on the susceptibility pattern is prescribed, a longer duration of treatment (14 days instead of 7 days) probably contributes to a greater success rate. In addition, systematic monitoring of the development of antimicrobial resistance of H. pylori in the Netherlands seems appropriate.
ACKNOWLEDGEMENTS
The authors would like to express their gratitude to T.J. Donker who assisted in retrieving the indications for the endoscopy for the period 2012-2015.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES