KEYWORDS
Cost effectiveness, emergency department, HIV, screening
INTRODUCTION
Early identification of patients infected with the human immunodeficiency virus (HIV) has been associated with benefits for both the individual and public health.1-3 From a public health perspective, early identification provides the opportunity to change risk behaviour and allows for earlier initiation of combination antiretroviral therapy (cART). This so-called ‘treatment as prevention’ has been shown to prevent onward HIV transmission.1,4 Clinically, late presentation of HIV-infected patients (CD4 cell count 350 cells/μl) increases the risk of death in the first year after diagnosis tenfold and leads to a decrease in life expectancy of ten years.5 Early initiation of cART has been shown to decrease morbidity and mortality, resulting in a life expectancy equal to that of the general population.2,6
Recent data show that in the USA an estimated 13% of persons living with HIV are still undiagnosed.7 Worldwide 17.1 million people living with HIV do not know they are infected with the virus.8 In the Netherlands, by the end of 2014, 12-34% of HIV-infected individuals (depending on the method used9,10) are estimated to be unaware of their infection. This is higher than the goal set by the Joint United Nations Program on HIV/AIDS (UNAIDS) that 90% of all people living with HIV should be aware of their HIV status.11 Diagnosis of HIV infections and subsequent linkage to care should therefore be scaled up. From 2006 the Center for Disease Control and Prevention (CDC) has recommended routine HIV screening at emergency departments (EDs) in the USA.12 Using different screening methods in different countries (UK, USA and Spain), prevalence of HIV infection among ED patients varied from 0.28% to 2.3%.13-17 Several studies have indicated that screening for HIV is cost-effective when the background rate of undiagnosed infections is greater than 0.1%.18,19 In the Netherlands, with an overall estimated background rate of HIV infection of 0.2%,9 HIV screening according to an opt-out policy is already implemented at maternity clinics and sexually transmitted diseases (STD) clinics. The National Institute for Public Health and the Environment (RIVM) also recommends an active test policy, especially in high-risk groups and in patients with HIV indicator conditions such as pneumonia, herpes zoster, seborrhoeic eczema, tuberculosis and hepatitis B and C.20 The rate of HIV infections in Rotterdam and Amsterdam is, at 0.5 and 0.9% respectively, well above the threshold for testing.
To our knowledge, there is no evidence as to whether non-targeted HIV screening at Dutch EDs is cost-effective. This study is the first to explore HIV prevalence and risk factors for HIV infection at the EDs of three hospitals in the two largest cities in the Netherlands. Additionally, we evaluated whether this approach would be cost-effective.
METHODS
Setting
The cross-sectional multicentre study was performed in two Dutch tertiary referral hospitals: the Erasmus Medical Centre (MC) in Rotterdam and the Academic Medical Centre (AMC) in Amsterdam and one large general hospital, the Sint Franciscus Gasthuis (SFG) in Rotterdam. The participating hospitals are located in two big cities in the Netherlands and provide care for a large inner city population. The ED of the Erasmus MC sees 24,000 patients a year, the AMC 30,000 and the SFG 28,000. All EDs are staffed with emergency physicians, residents and consultants of the different medical disciplines and specialised nurses. The study was conducted between August 2014 and October 2015: eight weeks at the Erasmus MC (18 August 2014 to 16 October 2014), six weeks at the AMC (2 February 2015 to 14 March 2015) and 22 weeks at the SFG (4 May 2015 to 2 October 2015).
Patients
All patients who visited the ED were informed about the study by posters and folders. Patients ≥ 18 years of age who attended the ED and had a blood sample taken for clinical care were eligible and were asked to participate. Patients were included once in case of more than one ED visit during the study period. Patients were included after written informed consent was obtained, as was requested by the medical ethics board. Since an additional blood sample was needed for the study, opt-out testing was not possible. Patients were given the choice to participate, rather than to opt-out, classifying the method as active choice.21
We checked patients records and questionnaires (see below) to exclude known HIV positives from blood testing. All study participants at the Erasmus MC and the SFG and a random sample of 100 study participants at the AMC were asked to fill in a questionnaire (in Dutch or in English) covering demographic data and items regarding previous HIV testing, history of STDs, previous HIV indicator conditions such as pneumonia, herpes zoster, seborrhoeic eczema, tuberculosis and hepatitis B and C, (recreational) drug use and perceived risk of HIV transmission. At the Erasmus MC, unused stored blood samples (drawn for diagnostic purposes) of patients of whom no informed consent could be obtained were batch-tested anonymously. These batch-tested samples were not retraceable to patients. The study was approved by the Medical Ethics Board of the Erasmus MC (MEC-2014-205 / NL48384078.14 and MEC-2015-763).
Laboratory HIV test
HIV testing was performed with a third-generation screening ELISA for HIV antibodies combined with an ELISA for the p24 antigen. A positive ELISA test was confirmed with a Western blot. When the ELISA was positive and the Western blot negative, an HIV-RNA PCR was performed. Screening tests were performed in each of the three participating hospitals, confirmation tests for the SFG were performed at the Erasmus MC. An HIV Ag/ Ab assay was performed on Liason XL (Diasorin) at the Erasmus MC and the AMC, at the SFG an HIV Ag/Ab assay was performed on the Architect (Abbott).
When a test result was positive, patients were informed by an infectious diseases specialist and were offered linkage to care.
Cost-effectiveness analysis
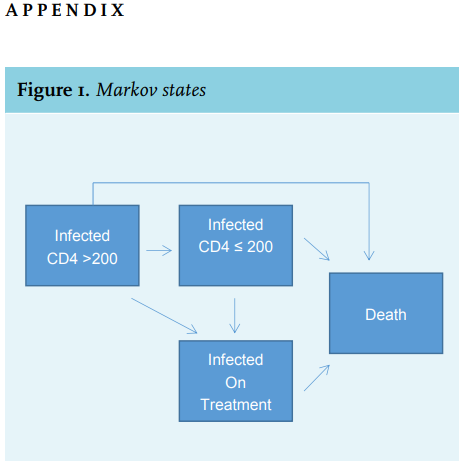
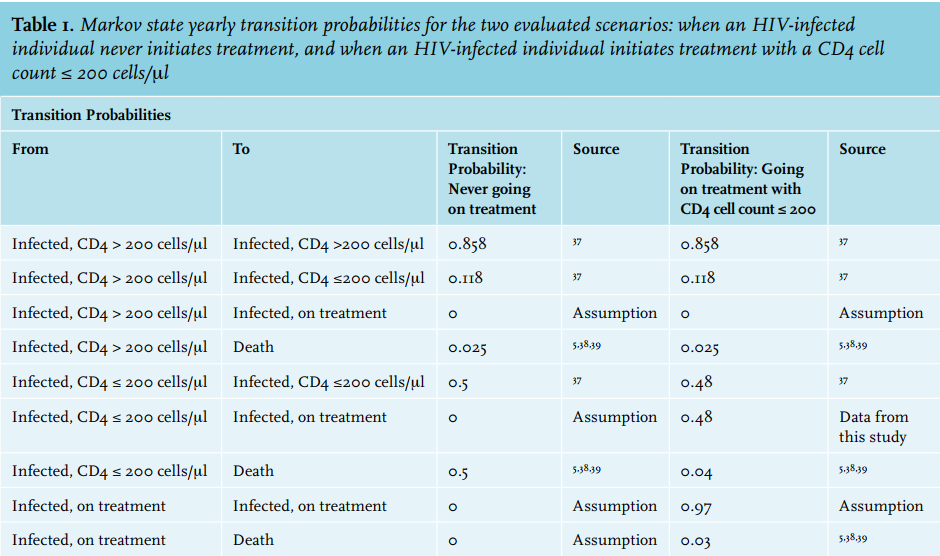
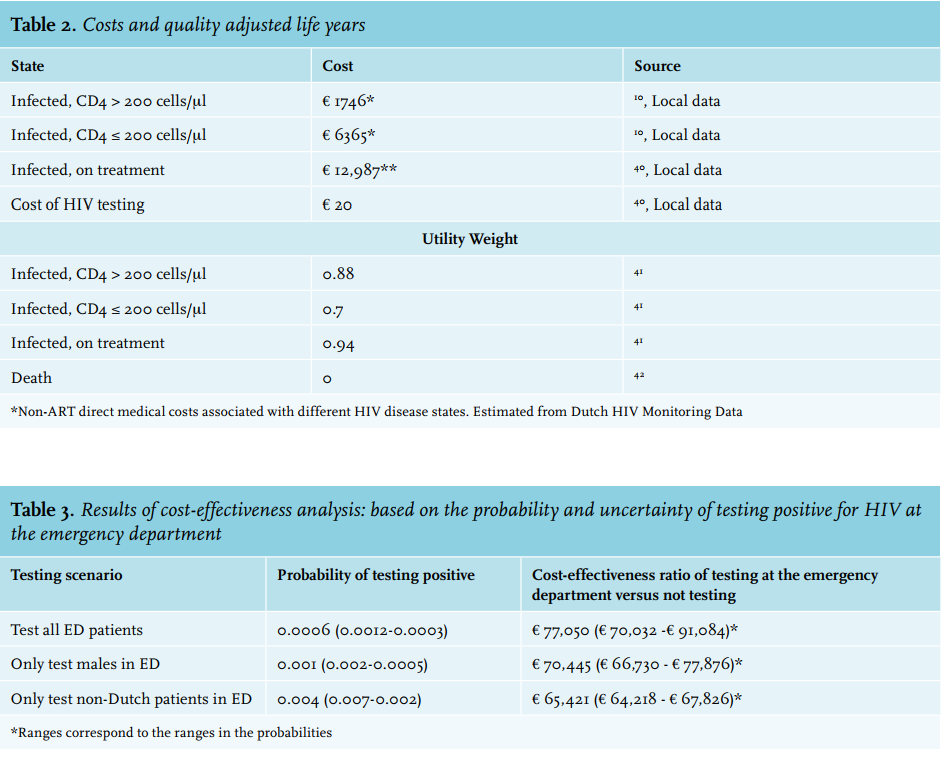
A Markov model imbedded within a decision tree was created to determine the cost-effectiveness of our HIV screening program (Appendix, table 1). The total costs and quality adjusted life years (QALYs) were calculated for two types of patients within the Markov model over a 20-year time horizon: for individuals who never underwent treatment, and for individuals who initiated treatment when the CD4 cell count dropped below 200 cells/μl. Four disease states were included: infected patients with CD4 cell count > 200 cells/μl, with CD4 cell count ≤ 200, infected patients on treatment, and death (Appendix, figure 1 and table 2).
We varied the probabilities that someone would test positive at the ED and reported the results for each of these probabilities based on the results of our study. We ranged the probability that an individual would test positive between half of the cases we identified to double the number of cases that we identified. We assumed that the uptake of treatment of those who test positive would be 99%. All costs and QALYs were discounted at 3% per year. Incremental cost-effectiveness ratios (ICERs) below € 20,000 were considered cost-effective in this analysis.22
Statistics
Based on the prevalence in other studies we assumed an HIV prevalence of 0.5% at the emergency departments in urban areas. We estimated a number to test of 4000 patients considering a confidence level of alpha = 0.05 and a power of 0.80. Analysis was performed with SPSS (IBM SPSS Statistics 21).
RESULTS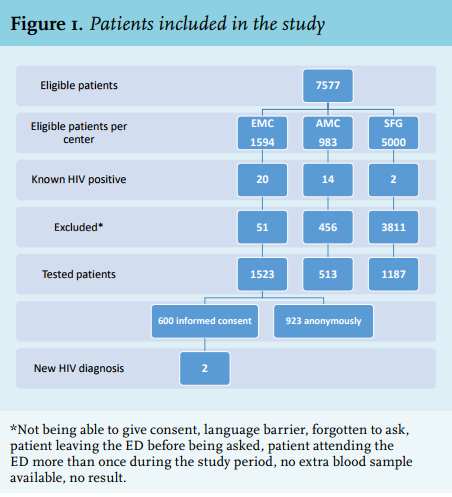
HIV prevalence
A total of 7577 patients were eligible during the study period and 3223 patients were tested, resulting in an inclusion rate of 43% (figure 1). At the Erasmus MC 600 of 1594 eligible patients consented to participate in the study (38%), at the AMC 513 of 983 eligible patients (52%) and at the SFG 1187 of 5000 (24%). Reasons for not participating were, amongst others, not being able to give consent, language barrier, forgotten to ask, patient leaving the ED before being asked and/or patient attending the ED more than once during the study period. The baseline characteristics are shown in table 1. The median age was 57 years and slightly more males than females were included. The majority of patients were of Dutch origin. First-generation immigrants predominantly originated from Surinam and the Caribbean and other European countries.
Two patients (0.06%) were newly diagnosed with an HIV infection, both in the Erasmus MC, and 36 patients were already known to be HIV infected and under the care in an HIV treatment centre. A total of 923 participants from the Erasmus MC, without informed consent, were tested anonymously and none tested HIV positive.
At the Erasmus MC and the AMC the percentage of HIV-infected patients seen at the ED (1.38% (22/1594), including the two newly diagnosed) and 1.42% (14/983)) respectively was comparable. At the SFG 0.04% (2/5000) of patients attending the ED were known to be HIV positive.
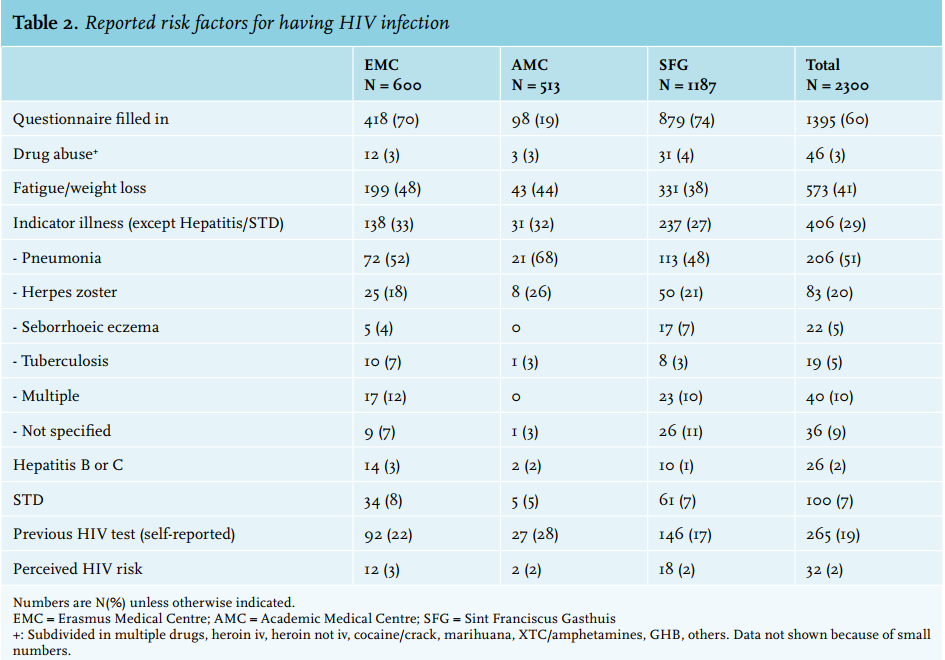
Of all patients visiting the ED who filled in a questionnaire, 2% reported a perceived risk for HIV transmission and almost 20% of all patients reported previous HIV testing (table 2). Reported illicit drug use was low (3% of the population) and intravenous drug use was not reported at all. Symptoms of fatigue and/or weight loss were present in 41% of patients and 29% of patients reported having had an HIV-indicator condition at any time. Most frequently reported HIV-indicator conditions were pneumonia and herpes zoster. If we had only tested patients with one or more risk factor, the HIV prevalence would have been nearly 0.2% (2 out of 1151 reported risk factors). 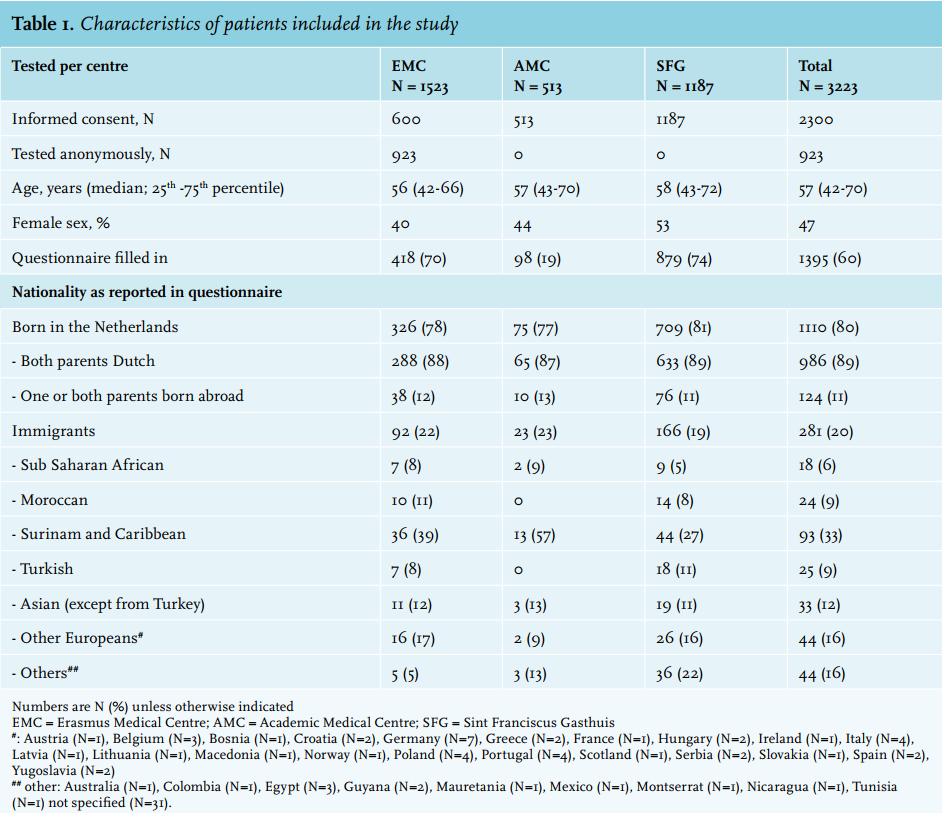
Characteristics of newly diagnosed patients
The two newly diagnosed HIV-infected patients were both heterosexual, older, male patients of non-Dutch origin, who had never had an HIV test. The first, a 50-year-old Cape Verdean, presented with a minor head injury, walking difficulties and bradyphrenia. His medical history was remarkable for pulmonary tuberculosis in 2006 and herpes zoster infection in 2013. The CD4 cell count at presentation was 170 cells per μl. After the HIV diagnosis, his cognitive dysfunction was thought to be secondary to HIV encephalitis/dementia based on MRI and lumbar puncture results and antiretroviral therapy was started. The second patient, a 73-year-old man from Spain, presented with cognitive dysfunction, hyponatraemia, leukopenia, and thrombocytopenia. His medical history was remarkable for syphilis in 1984 and 1995; in 2003 he was lost to follow-up during analysis for neurosyphilis. In 2013 and 2014 he was diagnosed with herpes zoster. The CD4 cell count at presentation was 80 cells per μl. Cerebral MRI showed atrophy and white matter abnormalities, a lumbar puncture was negative for HIV virus, syphilis and JC virus, and antiretroviral therapy was started.
Cost-effectiveness analysis
Non-targeted HIV testing at the ED is not cost-effective. Our study, where two patients out of 3223 participants tested positive, led to an ICER of € 77,050 per QALY gained, more than triple the current Dutch threshold for cost-effectiveness. If four patients had tested positive, the ICER would have decreased to € 70,032 per QALY gained. If just one patient had tested positive, testing at the ED would become far less cost-effective at € 91,084 per QALY gained. Even if testing had been targeted to those who are demographically more likely to test positive (i.e. only men over the age of 45 years and of non-Dutch origin, like the two newly HIV-diagnosed patients), the ICERs would have remained above € 60,000 per QALY gained (Appendix, table 3).
DISCUSSION
We showed that it was feasible to achieve an uptake of 40-50% of non-targeted HIV testing in two tertiary referral hospitals and one general hospital in the two largest cities of the Netherlands. The HIV prevalence in the population is 0.5% in Rotterdam and 0.9% in Amsterdam and the estimated HIV prevalence among undiagnosed persons 0.21% and 0.12% respectively.9 In our study, however, only two patients were newly diagnosed with an HIV infection (0.06%). Both patients were at risk for HIV infection and targeted or diagnostic HIV testing could have been performed at an earlier stage. The non-targeted HIV testing at the ED was not cost-effective at more than three times the current threshold for cost-effectiveness, which suggests that targeted screening programs to those with identifiable risk factors may be more effective.23
In our study, patients were offered HIV testing and had an active choice to participate rather than to opt-out. The inclusion rate was 43%. In a randomised clinical trial, inclusion of patients in an opt-out strategy was 66%, nearly 15% higher than in an active choice strategy (51%).21 The prevalence of HIV infection that we found in patients visiting the ED is in line with other studies, but the percentage of newly diagnosed patients with HIV infections (0.06%) was lower.13-17,23 In studies from the USA and France percentages of 0.52%, (range 0.14-1.7%) have been reported,23 0.08% in Ireland,24 0.14% in France25 and 0.4% in Spain.26
Our low percentage of new HIV infections may be due to the various intervention strategies already implemented to increase testing rates in the Netherlands, such as opt-out screening among pregnant women and in STD clinics with an uptake of more than 99%, guidelines for repeated HIV testing of men who have sex with men (MSM),27 as well as internet facilities for HIV testing and partner notification.9 Since it is not clear what preventive strategies are implemented in the settings in which the non-targeted HIV testing studies were performed, results of studies cannot be easily compared. The same holds true for the heterogeneity of patient populations and how the screening was implemented.21 Hsieh et al. showed that HIV infections are more prevalent among patients who were not offered or declined HIV testing compared with those who opted-in.15 However, in our study, HIV prevalence in the group in which no informed consent could be obtained (the 923 patients in the Erasmus MC tested anonymously), was not higher than in those who opted-in.
Another reason for the low prevalence of undiagnosed HIV infections in this study could be that the ED population is not representative of the inner city population. In the two tertiary referral hospitals a large percentage of patients are living in rural areas and predominantly of Dutch origin. Implementation of non-targeted screening is difficult.28-30 Barriers towards implementation and sustainability include costs, the effect on patients’ length of stay at the ED, and staff to perform testing and deliver results.31-33 Therefore, targeted test strategies aimed at patients with identifiable risk factors have been evaluated in the USA, the UK and Spain. Two studies showed that targeted testing was associated with identification of more new HIV infections when compared with non-targeted testing,26,30 whereas another study failed to demonstrate this benefit.34 In our study, 3% of the patients migrated from an HIV endemic area, 29% reported having had an indicator disease and only 2% of the patients indicated that they perceived having a risk for HIV transmission. Indeed, both of the newly diagnosed HIV patients belonged to the high HIV risk group of migrants from a country with a high prevalence of HIV or having had multiple sexually transmitted diseases.
The cost-effectiveness analysis based on the identification of the two patients with HIV infection resulted in an ICER of € 77,050 per QALY gained. It is likely that testing for HIV in the ED is even less cost-effective than we found in our study. We assumed that patients who are not tested at the ED will never test positive and die without a diagnosis. It is likely, however, that these patients would have presented and subsequently tested positive before death, making HIV screening at the ED even less cost-effective. As it is unknown what would have happened to these patients if they had not been diagnosed, we have chosen to compare them to the worst case scenario of death without diagnosis. Taking HIV transmission into account, in the UK annual HIV testing of all adults was calculated to cost £ 67,000 - £ 106,000/QALY gained, assuming that 25% of people living with HIV are undiagnosed.35 Thus, it seems that non-targeted HIV testing will only be nearing cost-effectiveness when the prevalence in the population is high or the percentage of undiagnosed people living with HIV is much higher than the 12-34% in the Netherlands. Of note, if annual testing was only offered to MSM, patients with intravenous drug use and people from HIV-endemic countries, with one-time testing for all other adults, then the costs would be £ 17,500/QALY gained,35 again suggesting targeted testing is preferable from a cost-effectiveness point of view. All studies suggest that to identify a few newly diagnosed patients, thousands of patients need to be screened.23
Our study has a number of limitations. First, we were not able to estimate the exact refusal and incidence rates, since patients not consenting consisted of patients not being offered the test at the ED, patients being not able to consent and patients refusing the test. It is also possible that the exclusion of these patients may have influenced the HIV prevalence, but our inclusion percentage is higher than in many other studies.23,32,33,36 Moreover, we did not find additional HIV infections in the 923 patients who were anonymously tested after failing to consent to the study. Second, due to practical problems and financial constraints, the inclusion procedure, the use of the questionnaire and anonymous testing of non-participants differed between the participating hospitals. It is unlikely that this influenced the outcome of this study, as positive test results were very low in all groups.
Due to the same reasons as mentioned above we did not succeed in inclusion of the calculated number of patients needed. Finally we did not get feedback about the acceptability of HIV testing in this setting.
CONCLUSION
In conclusion, non-targeted HIV testing in two urban areas in the Netherlands had a low yield of new HIV infections and was not cost-effective. Our data suggest that targeted HIV testing may offer an alternative approach to decrease the number of not yet diagnosed people living with HIV. According to the recommendations by the RIVM we suggest HIV testing in people presenting at the ED with an HIV indicator disease (pneumonia, herpes zoster, seborrhoeic eczema, tuberculosis and hepatitis B and C or STD), especially in patients from high-risk groups (MSM, immigrants and illegal drug users).
DISCLOSURES
Funding for this study was received from the AIDS Fonds. Trial registration number: NTR 4690.
REFERENCES