KEYWORDS
Sepsis, SIRS, anti-infective agents, antibiotics, inappropriate subscribing, stewardship
INTRODUCTION
Over the last decade, sepsis has been increasingly recognised as a major cause of death. After Rivers‘ publication and the start of the Surviving Sepsis Campaign, early detection and treatment has become a general endeavour with a special focus on the early administration of antibiotics.1 It should be noted that current evidence regarding early treatment with antibiotics was founded on studies including only patients with severe sepsis (mostly needing ICU treatment) or septic shock.1-4 However, in the effort to avoid delays in identifying sepsis many emergency departments (EDs) have started using the criteria of systemic inflammatory response syndrome (SIRS) and a clinical suspicion of infection as a way to screen their patients. The difficulty in identifying severe sepsis is that testing for organ damage (for example: renal function) takes time, whereas the recommendation is to treat severe sepsis within one hour (2012 Sepsis Guidelines5 ). Under the presumption that this waiting time may harm the patient, patients are increasingly treated with antibiotics without awaiting (all) the test results.
The Surviving Sepsis Guidelines of 2004 recommended administration of antibiotics in patients with severe sepsis or septic shock. The 2008 guideline did not give guidance as to how patients should be screened, but the 2012 guideline recommended screening of potentially infected seriously ill patients. The proposed instrument to screen for severe sepsis was an instrument based on SIRS criteria and clinical judgment, which was, however, only validated in ICU patients.3
From the very start, the SIRS criteria were criticised as defining condition for sepsis and recent publications refuelled the discussion.6-8 In February 2016, sepsis was redefined, removing the SIRS criteria and adding that the term sepsis had to be reserved for patients with severe organ dysfunction. The term ‘severe’ sepsis was dismissed and replaced by sepsis-3 and septic shock.9 However, SIRS criteria are still in use in clinical practice.
This study was undertaken to evaluate current practice and study the likelihood of bacterial infection in patients treated for sepsis in the ED according to the SIRS criteria. To address issues regarding antimicrobial stewardship, duration of antibiotic therapy was also evaluated.
METHODS
Study design and setting
A retrospective analysis was conducted using a cohort of consecutive adult patients presenting to the ED of the Albert Schweitzer Hospital (a large teaching hospital in Dordrecht, the Netherlands) from 1 January to 30 June 2011.
Inclusion
Patients diagnosed with sepsis (2008 definition) according to two or more SIRS criteria and a clinical suspicion of an infection, as assessed by the resident or ED physician, who received antibiotics upon admission were eligible.
Data collection
Data regarding vital parameters were extracted from the standard protocol form if completely filled out. All additional and missing data were extracted by hospital chart review. If more than one measurement of parameters was done in the ED, the most aberrant measurement was used in the analysis (the lowest BP recorded in the ED, or the highest respiratory rate or pulse). The primary investigator, as well as authors Spruyt and Huisman, performed the data extraction. The primary investigator then checked the data and in case of doubt regarding the primary outcome measures the case was discussed between the primary investigator and Dr. Levin until consensus was reached. Consensus was reached in all 37 patients that were discussed.
Definitions
The definitions for SIRS, sepsis, severe sepsis, sepsis-induced hypotension and septic shock were derived from the guidelines of the Surviving Sepsis Campaign in 2008. For the sake of clarity, in this article sepsis conform the old criteria will be referred to as sepsis and if referring to the new definition, sepsis-3 will be used.
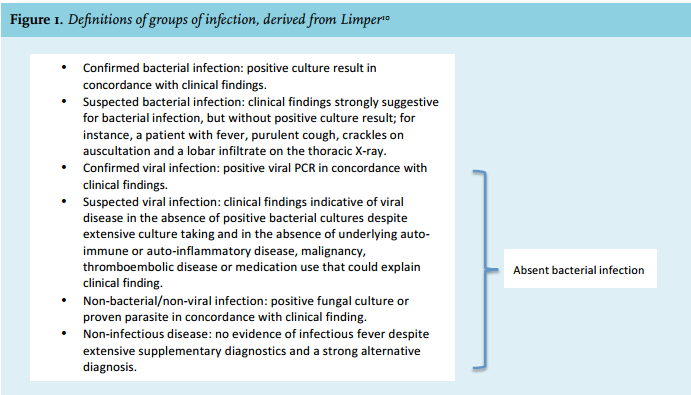
The criteria to define confirmed or suspected bacterial infection were derived from an article by Limper,10 as displayed in figure 1. In addition to these criteria another criterion, as found in previous literature, was added for further clarification of suspected bacterial disease: ‘Clinically documented infection: presence of gross purulence or an abscess (anatomical and/or by imaging and/or histological evidence), which may not be microbiologically documented if the culture remains sterile due to antibiotic therapy.’11
Outcome measures
Primary outcome measures were the number of patients with confirmed or suspected bacterial infection as assessed by the primary investigator using predefined criteria (stated above) and days of antibiotic use in these patients. Secondary outcome measures were severity of sepsis, rate of ICU admission, and mortality.
Data analysis
Results are expressed as mean ± standard deviation (SD), or median ± inter-quartile range (IQR) depending on normality of the data. Comparison between patients with and without bacterial infection was performed using the X2 test for categorical variables and the Students t-test (equal variances) or nonparametric Mann-Whitney U test for continuous data with non-normality. Statistical analyses were carried out using IBM SPSS 22.0.0 for OSX (SPSS, Chicago, IL). Missing data were excluded list-wise.
Ethics
The local institutional ethics review board approved the study design and a waiver for the retrieval of informed consent was obtained.
RESULTS
Patients and likelihood of bacterial infection
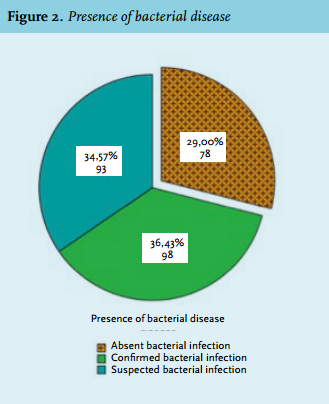
From 1 January 2011 to 30 June 2011, a total of 269 patients were diagnosed with sepsis (2008 definition) in the ED and received antibiotic treatment in the ED. Table 1 shows the baseline characteristics and main outcome measures. Retrospective analysis of clinical signs, cultures and other investigations using predefined criteria10 (figure 1) showed a confirmed bacterial infection in 98 (36%) patients, of whom 51 patients had bacteraemia. In addition, 93 patients (35%) were classified as suspected bacterial disease without microbiological proof. A total of 78 patients (29%) did not have objective evidence of bacterial disease. Amongst them 21 suffered from proven or suspected viral infection. Figure 2 illustrates the proportions. 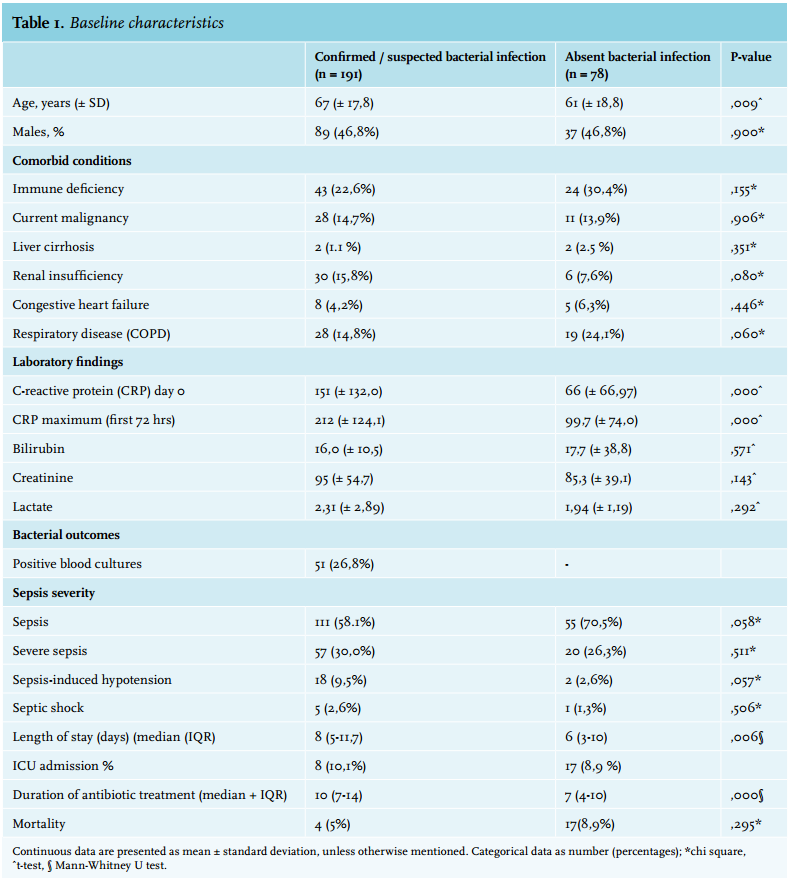
Severity of illness
In total 71% of patients, identified with sepsis in the ED, were likely to have bacterial infection. In the group with bacterial infection, the largest proportion (58%) fulfilled criteria for sepsis, 30% fulfilled criteria for severe sepsis, and only 9.5% showed sepsis-induced hypotension. A small percentage (3%) suffered from septic shock. This means that the largest proportion of the patients identified with bacterial infection (58%) would probably not fulfil the current sepsis-3 definition, although mental status was not documented reliably in all patients.
Factors associated with patients without bacterial infection
As shown in table 2 no significant differences in sex or comorbidity between patients with and without bacterial disease were established. The patients with bacterial disease were significantly older compared with the group without bacterial disease (p = 0.014). C-reactive protein at day 0 and day 3 was significantly higher in patients with bacterial disease than those without (p < 0.001 in both cases).
The number of SIRS criteria was significantly associated with the presence of bacterial disease. The odds ratio of having a bacterial infection was 2.32 (CI 1.3-4.3) if all four SIRS criteria were met in comparison with ≤ 3 criteria. The mean arterial pressure was significantly lower in the group with proven infection (p = 0.012), even though this was not reflected in the systolic blood pressure, but rather in the diastolic blood pressure. Leucocyte count was significantly higher in the group with bacterial infection (p = 0.001). Unexpectedly, patients with bacterial disease had a lower pulse than patients without a bacterial disease (p < 0. 001). Taking into account the severity of sepsis, the patients with more severe forms of sepsis (severe sepsis, sepsis-induced hypotension or septic shock) were significantly (p = 0.046) more likely to have bacterial infection compared with the group with sepsis alone.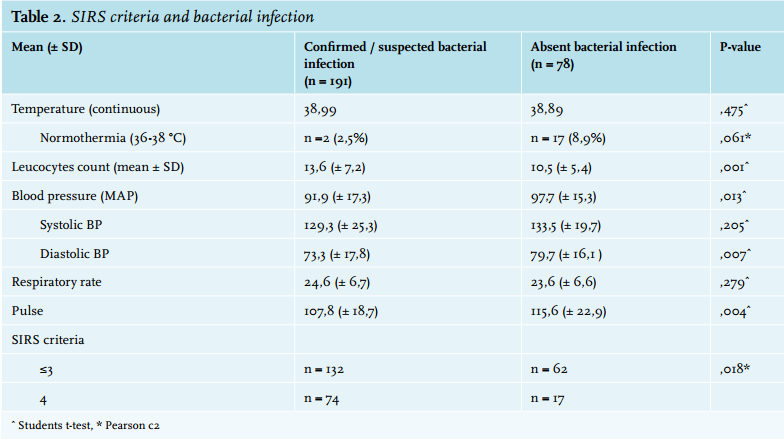
Alternative diagnosis in patients without bacterial infection
To further understand how patients become misdiagnosed as possible sepsis we carefully studied the alternative diagnoses in the residual group (table 3). The most frequent alternative diagnosis was exacerbation of chronic obstructive pulmonary disease (COPD) with or without viral respiratory infection (n = 26). Congestive heart failure (n = 7), neutropenic fever (n = 5), pulmonary embolism (n = 4 ) and viral pneumonia due to H1N1 influenza (n = 4) were the most prevalent alternative diagnoses, apart from quite a large group (n = 15), in which no clear diagnosis was made. 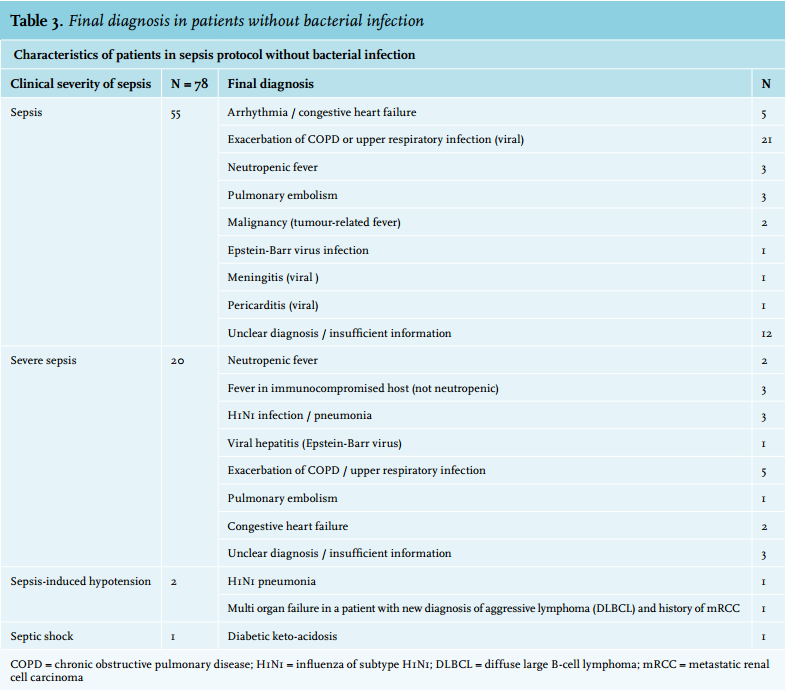
Antibiotic use
Data regarding duration of antibiotic treatment were available for 251 patients. In the remaining patients, data could not be retrieved, for example due to transfer to another hospital.
The median duration of antibiotics for all patients was 9 days (IQR 3-15), but median 11 days ( IQR 7-14) in patients with bacterial infection and 7 days (IQR 4-10 days) in patients without bacterial infections as displayed in table 4.
The most frequent infection was respiratory infection, which was treated for a median of 10 days. This is remarkable as evidence has shown that shorter treatments are safe and effective.12-14
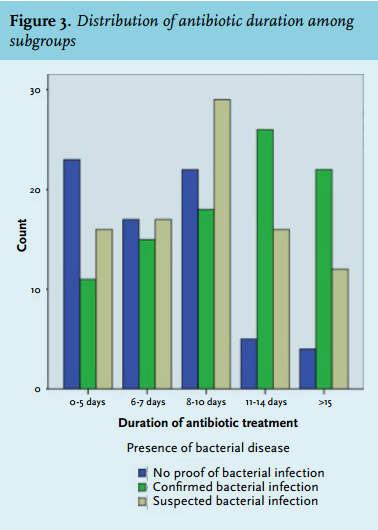
Antibiotics were stopped in the first 5 days in only 23 (32%) of the patients without bacterial infection, see figure 3 for more information. In this group antibiotic duration was significantly longer (p = 0.037) in patients with COPD in relation to patients with other comorbidities (current malignancy, congestive heart failure, liver cirrhosis, chronic renal insufficiency). Median duration was shortest in patients with confirmed or suspected viral disease (median 3 and 4 days, IQR 1-10.5 and 1.5-7.5).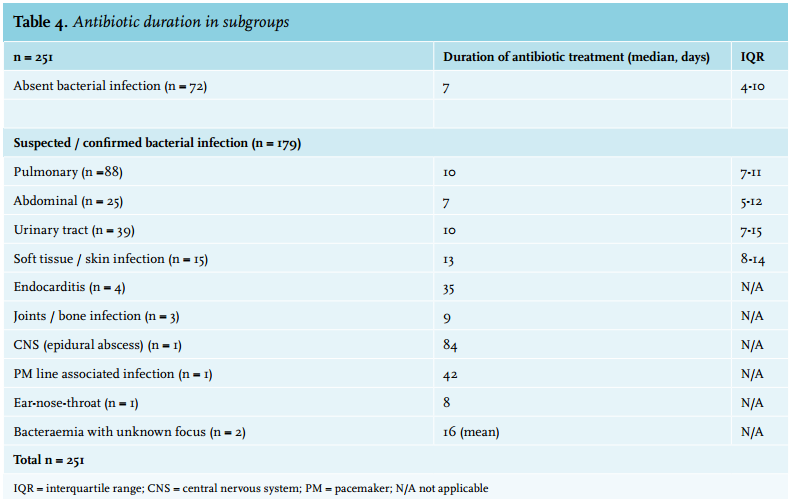
DISCUSSION
This study demonstrates that in almost 30% of the patients with suspected sepsis in the ED no objective evidence of bacterial disease could be found. This puts patients at risk of overtreatment with antibiotics. This finding is in concordance with an earlier report of patients admitted to the ICU with a diagnosis of sepsis,15 in whom no evidence of bacterial infection could be found in 13% and only a possible infection could be established in 30%. In spite of the improved outcome of patients treated early with antibiotics for severe sepsis or septic shock, this antibiotic overtreatment in patients with sepsis is a very important finding and often underreported. It is of paramount importance to establish that patients included in sepsis research (on clinical suspicion) are in fact suffering from an infectious disease. Future research will have to report infectious outcomes in detail, to enable correct interpretation and extrapolation of the results.
Antibiotic treatment within the hour
The most important intervention in severe sepsis treatment in the last decades, next to fluid treatment, has been the emphasis on early antibiotic treatment. The problem in every ED, however, is that signs and symptoms of severe sepsis can be deceiving or occult. Postponing antibiotic treatment whilst awaiting basic test results (i.e. kidney function, chest X-ray) does not fit well within the one-hour target which has been outlined by the sepsis guidelines. The benefit of early antibiotic treatment has been established in suspected sepsis patients admitted to the ICU.1-4,16-18 Two other studies showed benefit of early antibiotic treatment in ED patients but selected only patients with sepsis and organ dysfunction or patients with hypotension/ hyperlactataemia (lactate > 4 mmol/l).19-21 However the largest group identified by our screening did not have organ dysfunction, and only about 10% needed ICU care. This means that more than half of our patients could have awaited basic test results (which might have raised suspicion of alternative diagnoses), thus allowing more time to consider if antibiotic treatment is really indicated. In pneumonia, studies have shown that treatment within four hours is safe.22 This leaves more than enough time for at least a chest X-ray and lab results to come in.
Antibiotic treatment in the ED within the hour should generally be reserved for critically ill patients, patients deteriorating quickly, or specific patient groups such as neutropenic patients. Future research will hopefully guide us further as to which risk-stratification score (Modified Early Warning Score (MEWS), National Early Warning Score (NEWS) or Quick Sequential Organ Failure Assessment (qSOFA) is most helpful with identifying patients at risk of deterioration or death.
Duration of antibiotic therapy
Overall the duration of antibiotic therapy was long in our cohort. This may reflect local standards or may be because our patients were selected in 2011.
Of concern, patients in our cohort without evidence for bacterial disease were treated with antibiotics for a median duration of 7 days, pointing to overuse. Antibiotic treatment was stopped in the first 5 days in only 32% of the patients with negative culture results. Several reasons for the prolonged use of antibiotics can be suggested.
1. The ED presumptive diagnosis of sepsis makes it hard to stop antibiotics despite negative cultures. This could be due to cognitive errors such as the tendency to stick to first impressions (anchoring error) and the tendency to stick to prior diagnoses (confirmation bias) despite conflicting evidence.
2. The large number of patients suffering from COPD in this subgroup, in whom antibiotic treatment is often given despite negative cultures. Even so, evidence is mounting that shorter regimens are safe for bronchitis and pneumonia.12-14
3. Clinical improvement of patients after admission and starting antibiotics.
4. Fear of undiagnosed bacterial disease by physician or patient.
5. Fear of inducing antimicrobial resistance if antibiotics are stopped prematurely. This is a theoretical problem which is hard to prove or refute in practice. Though widespread, it has been challenged over recent years. New research in the area of pneumonia shows that shorter treatment regimens are safe without signs of inducing microbial resistance.12-14 A review in 2016, looking at de-escalation of antimicrobials, concluded that de-escalation appears safe and effective for certain conditions, but calls for further, high-quality, research.23 All in all, de-escalation seems safe, and if antibiotics are used for too long for fear if inducing resistance, this might actually constitute antibiotic overuse.
Limitations
Limitations of the study are its retrospective character and the single-cohort design in a single hospital. Another point of concern is the allocation of patients to groups suffering from proven/ suspected or no bacterial disease. It has been pointed out before that many patients suffering from a bacterial infection (i.e. pneumonia) may not have positive culture results. A patient suffering from urosepsis may have negative cultures due to prior treatment initiated by the primary care physician. In these patients, it is hard to determine in retrospect if they were truly suffering from bacterial disease. We have put a lot of effort into accurately determining the correct group for each patient, but in some cases it is inevitable that discussion will always remain. However, as this reflects daily practice it does not reduce our concerns of overtreatment and the protracted duration of antibiotic use.
Future investigations evaluating the sepsis campaign or regarding screening in the ED should report microbiological outcomes and include overuse and possible harm of antibiotics as endpoint to avoid a singular focus on benefits of early sepsis treatment.
Relevance and recommendations
With the new sepsis-3 definition, treatment within one hour based only on SIRS criteria cannot be substantiated. However, it is still difficult to know which patients in the ED have to be treated within the hour. qSofa was introduced as an instrument to identify patients with sepsis who are likely to fare poorly and should thus be treated early with broad-spectrum antibiotics.9 This is an important step forward. However, it was noted that early treatment should not be limited to patients with a positive qSofa. Several reports have been made since, but acceptance of qSOFA is not universal. One investigation showed poor sensitivity of 63% for qSOFA in the ED population.24 The same report found that the NEWS was the most accurate tool in predicting in-hospital and ICU mortality. In the UK, use of NEWS is mandatory and qSOFA has not been implemented. Since the best way to identify a septic patient in the ED is still under discussion, this study offers valuable information regarding the use of SIRS criteria.
With respect to antibiotic duration and de-escalation, the current guidelines recommend daily reconsideration of antibiotic therapy. Unfortunately, only a few studies have been performed regarding the safety of early de-escalation in patients outside the ICU. More research is needed in the area of de-escalation in suspected sepsis patients.
CONCLUSION
Sepsis detection in the ED is a continuous challenge. This study shows that early recognition of sepsis using SIRS criteria leads to over identification of sepsis. More than half of the patients suspected of sepsis would probably not fulfil the current sepsis-3 definition, and almost 30% did not have objective evidence of a bacterial infection. In some of the patients without bacterial infection, awaiting basic tests might have confirmed an alternative diagnosis and antibiotic treatment could have been avoided.
In a significant proportion of patients, empiric therapy was justified but with a median duration of therapy of seven days de-escalation should have been much more rigorous.
DISCLOSURES
All authors declare no conflict of interest. No funding or financial support was received.
REFERENCES