KEYWORDS
Dialysis, relative contraindications, survival, transplantation
INTRODUCTION
Current guidelines for the evaluation of renal transplant candidates consist of various recommendations with relative and absolute contraindications for transplantation.1,2 These guidelines try to balance the possible advantages of transplantation with the risk of the surgical intervention and immunosuppression. Additionally, the selection of transplant candidates has to take into account the shortage of available organs by trying to avoid allocating scarce organs to patients with a short life expectancy or a high risk of early graft failure.
However, even in patients with severe comorbidity, the life expectancy may still be significantly better after transplantation compared with remaining on dialysis.3-5 Previous studies have reported that kidney transplant recipients have better health-related quality of life than transplant candidates maintained on haemodialysis.6-8 Transplantation is the treatment of choice for end-stage renal disease; it increases survival and quality of life, while being more cost-effective than dialysis.9-12
There is a considerable variation between Dutch transplant centres concerning the acceptance of patients with relative contraindications for transplantation. A general consensus exists concerning the refusal of patients with severe disease limiting the life expectancy to less than five years.13 However, guidelines and medical practice are less clear with relative contraindications such as obesity, cardiovascular disease and old age. Obesity is one of the major reasons for not putting patients with end-stage renal disease (ESRD) on the renal transplant waiting list.14
Over the past years, the kidney transplant program of the Erasmus MC, Rotterdam has adopted a rather liberal policy to accepting transplant candidates with relative contraindications for transplantation. In the course of this approach, numerous candidates who were refused at other transplant centres were referred to our centre resulting in kidney transplantation in many of them.
The aim of this study is to describe and investigate the outcomes after kidney transplantation in these patients. Additionally, we were interested if these patients judged their quality of life as improved and whether they, in retrospect, are satisfied with the decision to undergo a kidney transplantation despite earlier contrary advice.
MATERIALS AND METHODS
Study design and endpoints
This investigation was a retrospective study that was designed to identify all patients referred from outside our adherence area. First, we identified all patients who had been referred from outside our regular referral area from January 2000 until March 2013. Those patients who had been declined for transplantation or wait-listing at other transplantation centres were included. We excluded patients with: missing information about the reason for declining transplantation, patients with combined liver-kidney transplantation, ABO incompatible transplantation, and patients who chose for our centre after acceptance at another centre. We used our electronic patient information system to identify the reasons for referral. Follow-up data were retrieved from the electronic patient information system and our own transplantation database. We recorded the type of transplantation procedure (living versus deceased donor), postoperative complications (e.g. wound healing problems, infections, cardiovascular complications etc.), long-term complications, renal function (creatinine, estimated glomerular filtration rate (eGFR)) at 3 and 12 months as well as patient and graft survival. Delayed graft function was defined as dialysis treatment performed within seven days after transplantation. As a representative control group we used all patients transplanted in 2010 who were primarily referred to our centre and we noted the duration of initial hospitalisation and additional hospitalisation in the first year after transplantation, wound problems, creatinine and eGFR after 3 and 12 months.
Additionally, the patients were interviewed to evaluate their perceived quality of life after transplantation and asked to compare their post-transplant situation with the situation before transplantation.
All clinical information obtained in the study was considered to be confidential and was used only for research purposes. Patient data were stored in an anonymised fashion. All patients participating in the quality of life questionnaire provided written informed consent. This study did not require institutional ethics committee review.
Statistical analysis
Patient characteristics, such as BMI, number of previous transplantations, as well as outcome measures were presented as means / medians ± standard deviation or interquartile range as appropriate. Hospitalisation duration, differences in creatinine and eGFR were compared with the t-test or the Mann-Whitney U-test as appropriate. Differences in categorical variables between the study and control group were analysed with the chi-square test. All analyses were performed using SPSS 21.0 and statistical significance was defined as p < 0.05.
RESULTS
Initially 30 patients, who were referred to our centre in the period from January 2000 until March 2013, were identified for inclusion in the study. Of these, six were excluded from the study because they had been referred to our centre because of live donor-associated problems. One additional recipient was excluded as she indicated that she had actively chosen to be transplanted at our centre and had not been denied transplantation at the initial centre. The 23 remaining patients were included (table 1). A total of 21 transplantations were performed from 2007 until 2013. The remaining two were performed in 2001 and in 2004. The group consisted of 16 male (69.6%) and seven female patients (30.4%). The majority were transplanted with a living-unrelated donor (39.1%). Various reasons for refusal at other centres were identified, such as obesity, malignancies, old age, hyperparathyroidism and overall poor condition. In six patients more than one reason for refusal was given in the decision letter. Obesity was the most important reason for refusal in seven patients (30.4%), with a BMI that ranges from 35.0-42.1 kg/m2. Five patients were denied transplantation because of malignancies in the past: a successfully removed renal cell tumour three years before transplantation, smouldering multiple myeloma, recurrent pheochromocytoma and focal segmental glomerulosclerosis, skin cancer and an ovarian carcinoma which was successfully treated with chemotherapy and surgery 14 years before, and a patient with an oesophageal carcinoma in 1990, which was successfully treated, but still had serious ongoing skin cancer with removal of multiple squamous cell skin cancers in the past.
The median age at the moment of transplantation was 54 years (range 44.0-61.0). At baseline, 14 patients had diabetes mellitus (60.9%) and 8 of the 23 patients (36.4%) had a BMI > 35 kg/m2. Three patients (13.0%) underwent a pre-emptive transplantation while 12 patients (52.2%) were on dialysis treatment for more than three years at the moment of transplantation. The median follow-up was 21.0 months (range 11.0-48.9) and two patients died in the follow-up period. One patient died ten days after the transplantation as result of a major stroke; another patient died 11 weeks after transplantation because of a cardiac arrest.
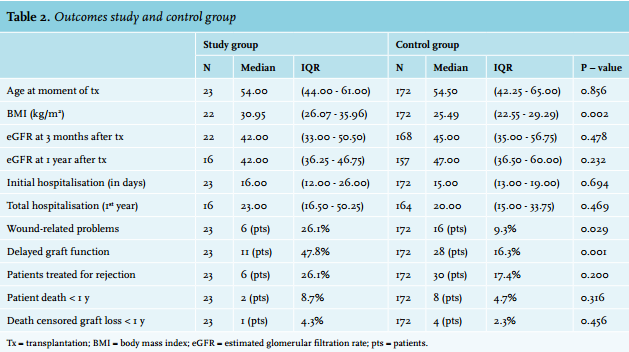
We compared our study group with a control group consisting of patients who were primarily referred to our centre and transplanted at our centre in 2010 (table 2).
Delayed graft function was seen significantly more often in the study population (p = 0.001) while the incidence of rejection treatment was not significantly different (p = 0.200). Immunosuppression consisted of induction with basiliximab plus tacrolimus and a mycophenolate mofetil (MMF) maintenance treatment. Steroids were withdrawn in all patients at three months after transplantation. There was no significant difference between the study and control group regarding mean second ischaemic time: 28.6 vs. 24.2 minutes respectively (p = 0.115).
The group of patients that had been declined at other centres had a significantly higher BMI as compared with the control group, 31.0 vs. 25.5 (p = 0.002), and the study group experienced more wound-related problems (p = 0.029): three patients in our study group had delayed wound healing, all without fascial dehiscence. They were seen frequently for wound inspection and within one year after transplantation all wounds had healed. One out of the three patients with delayed wound healing and one other patient experienced wound infections, which were treated with antibiotics and in one patient surgical exploration was required. After surgery the patient did well and the wound healed promptly. Interestingly, the patients with wound infections all had a normal BMI, but did have diabetes mellitus.
Kidney function one year after transplantation was comparable in both groups. Remarkably, there were no significant differences in rejection rate, patient death and death censored graft loss in the first year after transplantation.
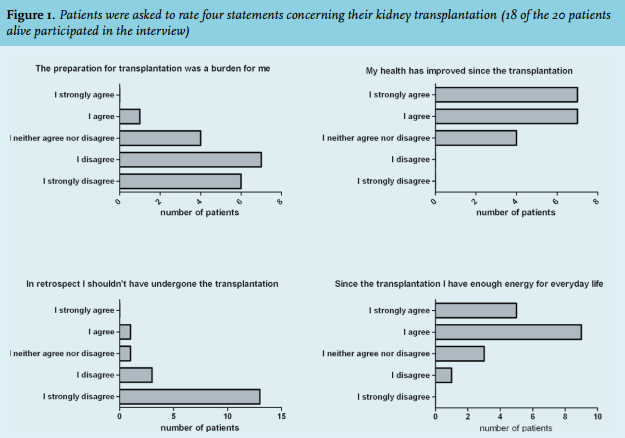
Next to the clinical follow-up, we were interested in how patients rated their quality of life and how they looked back at their transplantation (figure 1). Eighteen of 20 living patients were willing to participate in the interview. Before transplantation, patients mainly mentioned limitations in everyday life such as: not being able to work, not having enough energy to walk long distances, to do the daily shopping and housekeeping. Only one patient experienced the preparations for the transplantation as a burden, while 13 patients (72.2%) did not. Fourteen patients (77.8%) reported an improvement in their health since the transplantation, three considered their health to be unchanged after transplantation and one 23-year-old patient thought his health had worsened since transplantation: in the two years following transplantation he experienced multiple ischaemic strokes. Most patients reported feeling less tired and thought that their general physical condition had improved. A number of patients mentioned that the most important change was that dialysis no longer dominated their lives. Sixteen of the 18 patients (88.9%) who completed the questionnaire would choose for kidney transplantation again if they were in the same situation.
Only one patient felt that he would not undergo the kidney transplantation again, it was the same patient as mentioned above, mainly because of a negative change in the relationship with his living donor, and other family members. Fourteen patients (77.8%) reported a perceived improvement of their energy in everyday life.
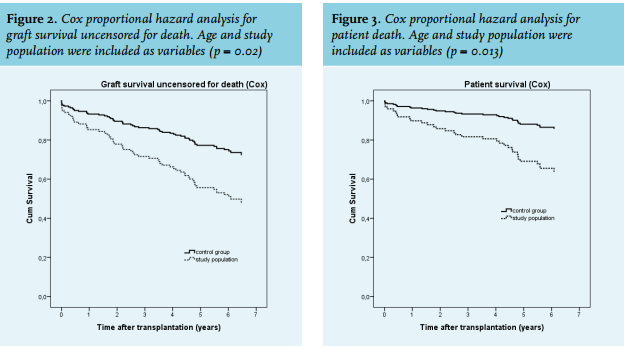
Additionally we performed a Cox proportional hazard analysis for the risk of death and graft failure uncensored for death. Age and study population were included as variables (figure 2). Our study population had a significantly higher relative risk for graft failure uncensored for death (RR: 2.3, CI: 1.1-4.5, p = 0.02) compared with the control group. The Cox analysis for patient survival showed that the study population had a significantly higher risk compared with the control population. (RR = 2.9, CI: 1.3-6.8, p = 0.013) (figure 3).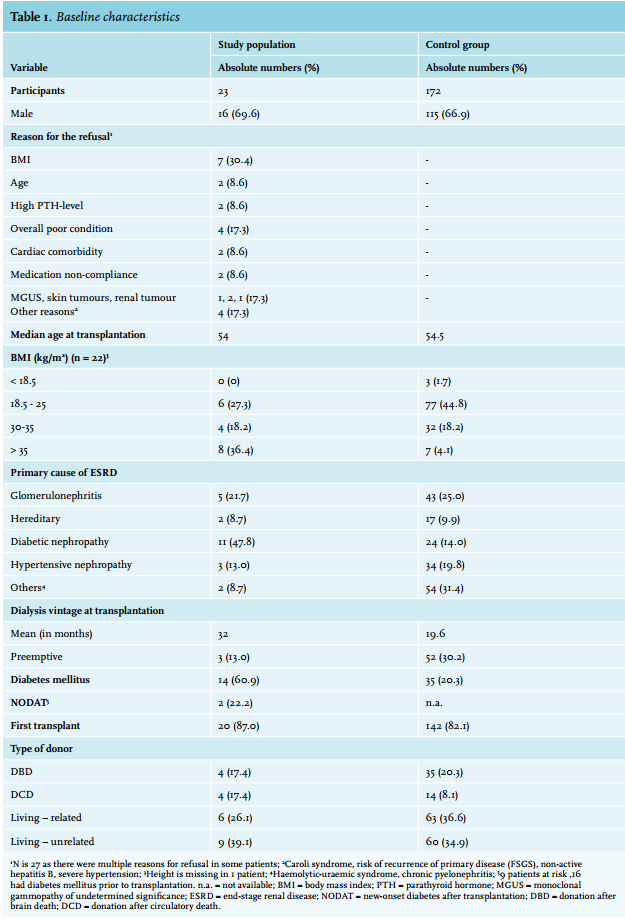
DISCUSSION
This study shows the outcomes of patients who were transplanted at our centre after they were denied access to transplantation at other transplant centres in the Netherlands. Of the 23 patients included, 20 are still alive and 19 have a functioning graft at a median follow-up of 21.0 months. Patients in the study group had significantly more wound-related problems when compared with the control group. However, the kidney function was not significantly different between the two groups. The length of the initial hospitalisation and total hospitalisation duration in the first year after transplantation was not significantly higher in the study group.
The ideal control group for this study would be a group with a similar risk profile, but who remained on dialysis. As we do not have a matched group on dialysis, it is difficult to make definite conclusions on the survival and morbidity of our patient population. However, it does seem safe to speculate that a survival rate of 86% after a median follow-up of 22 months is quite favourable in this group of ESRD patients with a large proportion of diabetes. It seems improbable that the mortality would have been as low if these patients had remained on dialysis.
In the study the amount of wound problems was significantly higher than our standard transplant population. This is probably explained by the higher BMI when compared with the control group, which is a well-known problem.15 However, these wound complications had all resolved within six months after transplantation and did not cause long-term morbidity. Transplantation seems to be an appropriate treatment for these patients in the study group and probably resulted in improved survival when compared with the initial decision to deny these patients access to transplantation.
BMI was a frequent reason for other transplant centres to turn these patients down. The number of obese kidney transplant candidates has been growing in the last years.15-18 Obesity is perceived as a relative contraindication for listing and receipt of renal transplantation and many transplant professionals have been reluctant to offer transplantation to obese candidates because of the risk of surgical complications after transplantation and poorer survival when compared with non-obese transplant recipients.15,16 However, the impact of obesity on renal transplantation has not been clearly defined.4 It has been shown that recipient obesity is associated with an increased risk for delayed graft function and local wound complications,15,19 which is in keeping with the findings in our study group. However, our patients felt that their quality of life was improved by transplantation and they did not report the wound complications as an important burden. Another impact of BMI/ morbid obesity (> 35 kg/m2 ) is longer hospitalisation compared with patients with a ‘normal’ BMI (20-25 kg/m2 ).18,19 We did not see a significant difference in hospitalisation duration when compared with the control group. However, the effect of obesity on hospitalisation may be masked by a relatively long standard length of initial hospitalisation in our program. Older age is another relative contraindication which is an important predictor of kidney transplantation outcomes. The demand for kidney transplantation among the ESRD population of 65 years and older is growing.20 Elderly recipients, > 65 years, experience more infectious complications, have a lower crude graft and patient survival and a higher risk of mortality, but experience less acute rejection.11,21 The patients in our cohort who were refused at other centres because of high age are all still alive with a functioning graft after a median follow-up of 21.0 months. We think that the transplantation was a suitable choice for these patients because of the expected high mortality22 on dialysis and the perceived improvement of their health after transplantation reported by the elderly patients in our cohort. Transplantation in older patients has been shown to be appropriate for a large proportion of elderly patients with renal failure.3,20
Malignancies in the recent past (< 5 years) was another reason for refusal. Two of the four patients identified had had a previous transplantation and one of them had recurrent skin tumours after his transplantation within our series. The other three patients did not experience malignant complications within the studied period. All four patients are still alive with a functioning graft.
Figure 2 shows graft survival uncensored for death in the study population of 50% after six years. This was significantly worse than the survival of the unmatched control group. However, as mentioned above, is seems reasonable to speculate that survival would have been poorer when these high-risk patients had remained on dialysis. A recent study of our group confirms that patients with extensive comorbidity enjoy a remarkably good graft and patient survival: 50% of those with the highest comorbidity score survived more than ten years after transplantation, while graft survival was not different from patients with lower comorbidity scores.23
Importantly, the interviews demonstrate an improvement of the perceived quality of life after transplantation and almost all patients were still content with the decision to undergo the transplantation despite contrary advice by another transplant centre.
One of the limitations of the study was the small sample size of our identified recipients. Another limitation is the retrospective nature of the analysis. Especially during the interviews, recall bias is a problem as the transplantations had often been performed several years ago. Additionally, the quality of life analysis may be biased due the fact that three patients had died and two patients refused to participate. As mentioned above we were not able to identify a suitable control group on dialysis. Furthermore, the follow-up period was limited. Despite these limitations, we feel that this study provides some insight into an important problem in kidney transplantation.
In conclusion, the acceptance of patients who were declined for kidney transplantation at other centres resulted in successful transplants with high patient satisfaction. Our findings indicate that our current criteria for the acceptance of transplant recipients are far from stringent and that individualisation and shared decision-making are important tools in this process.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES