KEYWORDS
Stroke prevention, atrial fibrillation, direct antithrombin agents, systemic embolism
INTRODUCTION
Atrial fibrillation (AF) is an important risk factor for thromboembolic events such as stroke and systemic thromboembolism. Oral vitamin K antagonists such as warfarin have been the treatment of choice in preventing thromboembolic events in patients with AF. However, frequent dose adjustment, slow onset of action, and monitoring of coagulation status, including multiple drug and food interactions, complicate routine use.
Therefore, several new direct oral anticoagulants (DOAC), including dabigatran etexilate, have been developed. Dabigatran etexilate is an oral prodrug that is rapidly converted by a serum esterase to dabigatran, a potent, direct, competitive inhibitor of thrombin (factor IIa). Dabigatran specifically and reversibly binds and inactivates not only free but also fibrin-bound thrombin, leading to a reduction in fibrin clot formation and platelet aggregation. As this agent acts differently to warfarin, the bleeding time and INR will often be normal. Dabigatran has an absolute bioavailability of 6.5%, 80% of the given dose is excreted by the kidneys and its serum half-life is 12 to 17 hours.1
Dabigatran was first approved by the European Commission and the US Food and Drug Administration to reduce the risk of stroke and systemic embolism in patients with nonvalvular atrial fibrillation. The RE-LY (Randomized Evaluation of Long-Term Anticoagulation Therapy) trial, a randomised trial comparing two doses of dabigatran (110 mg twice daily and 150 mg twice daily), given as a fixed dose without laboratory monitoring, with coumarin, showed similar or reduced rates for stroke or systemic embolism, without an increase in bleeding.1 Further, dabigatran has been studied and approved for the treatment and prevention of recurrence of deep vein thrombosis and pulmonary embolism as well.
Based on the pharmacokinetics and pharmacodynamics of dabigatran, a fixed-dose treatment without the need for coagulation monitoring has been advised. However, significant variations in plasma levels between patients have been described with the occurrence of thromboembolic events and bleeding in patients with dabigatran pharmacotherapy.2-4
In this report we describe a patient with nonvalvular AF with the formation of a left atrial thrombus and severe thromboembolic events after treatment with dabigatran.
CASE REPORT
A 60-year-old Caucasian male, BMI 28 kg/m2 , was known with persistent AF. Besides an episode of ultrasoundproven diverticulitis two years ago, the patient had no relevant medical history. In 1995, at the age of 40 years, the patient suffered from peripheral embolism in his right hand and a transient ischaemic attack in the right cerebral hemisphere based on newly diagnosed AF. After this, he was treated with acenocoumarol with a target prothrombin international normalised ratio of 2.5 to 3.5 without suffering bleeding or embolic complications. During those years, the patient had several recurrences of AF, which were treated with direct current cardioversions. In 2010, the patient underwent pulmonary vein isolation; during this procedure, the left atrium was severely enlarged with fibrotic areas. After ablation, the AF recurred and persistent AF was accepted. Five months before presentation, on the patient’s request, he switched from acenocoumarol to dabigatran 110 mg twice daily. The rationale behind this low dose of dabigatran was anticipating an increased risk for lower intestinal haemorrhage due to colonic diverticulosis and the fact that dabigatran 110 mg twice showed to be non-inferior to coumarin in the RE-LY trial.
At presentation, the patient complained of right calf pain and mild amnesia for four days. Physical examination showed a livid discoloration and cold right forefoot with a reduced posterior tibial pulse on the right side. No other abnormalities were found. The patient’s medication was dabigatran 110 mg twice daily, verapamil 40 mg twice daily and omeprazole 40 mg daily. He was reportedly compliant with his medication and he had no history of trauma, surgery, immobilisation or smoking. Family history was negative for clotting disorders. At admission he had a dabigatran level of 35 ng/ml, assessed to verify compliance, measured six hours after the last reported dabigatran intake. The estimated glomerular filtration rate using the Modification of Diet in Renal Disease (MDRD) formula was 49 ml/min/1.73 m2 and one day after fluid infusion 65 ml/min/1.73 m2. There were no other laboratory abnormalities and the dabigatran level was not measured before his current event. CT angiography of the legs showed acute thrombosis of the anterior tibial and posterior tibial artery. After intra-arterial thrombolysis, his symptoms improved slightly.
Transthoracic echocardiography showed a normal left ventricular function, an enlarged left atrium (63 ml/m2 ), but no cardiac source of embolism. However, subsequently, transoesophageal echocardiography demonstrated a large left atrial thrombus (figure 1, left panel). Magnetic resonance imaging of the cerebrum showed a small infarction of the posterior inferior cerebellar artery.
To exclude underlying malignancy, CT scans of the chest, abdomen and pelvis were performed, showing multiple small infarctions in the kidney and spleen. Risk factors for venous and arterial thrombosis were established, including protein S, protein C, antithrombin activity, factor VIII activity, lupus anticoagulant, anti-b2-glycoprotein antibodies, anti-cardiolipin antibodies, the platelet count, lipoprotein analysis, paroxysmal nocturnal haemoglobinuria analysis and DNA analysis for mutations in factor II and factor V. All were negative, only a dubiously positive lupus anticoagulant was noted, which we related to the presence of dabigatran in the sample. Due to the medical necessity of anticoagulation therapy, lupus anticoagulant presence could not be verified in a later state. The patient was hospitalised, dabigatran was ceased and we initiated treatment with enoxaparin 1 mg/kg twice daily and clopidogrel 75 mg once daily. Surgical removal of the left atrial thrombus was considered, but not performed. Except for a transient paresis of the left hand, no additional thromboembolic events occurred. The patient was discharged, after resumption of acenocoumarol (with INR range between 3.5-4.5) and continuation of clopidogrel. One month after presentation, a new transoesophageal echocardiography was performed, now demonstrating complete resolution of the left atrial thrombus (figure 1, right panel). The patient was discharged, after resumption of acenocoumarol and continuation of clopidogrel. After follow-up of 12 months, no recurrent thromboembolic events occurred. 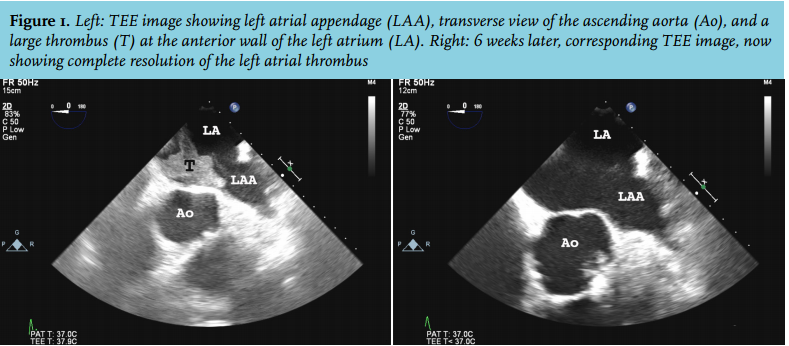
DISCUSSION
VKAs are effective for reducing the risk of thromboembolic stroke in AF patients.5 However, frequent laboratory monitoring and dosage adjustments are required, due to a narrow therapeutic window and multiple interactions. Recent studies have demonstrated that dabigatran is at least equally effective.6 Because of the claimed predictable pharmacokinetics, dabigatran was recommended at a fixed dose and does not require coagulation monitoring and/or laboratory test-guided dosage adjustments.7
Since the introduction of dabigatran, a few case reports have been published describing the occurrence of thromboembolic events in the setting of dabigatran pharmacotherapy. Sargento-Freitas et al. described a case of a 70-year-old female patient with an acute ischaemic stroke on dabigatran 110 mg twice daily. The dabigatran plasma peak concentration of confirmed therapy intake was 40.6 ng/ml. After dosage adjustment to dabigatran 150 mg twice daily, low peak concentrations persisted.3 Sharma et al. report two cases of large left atrial thrombi and occurrence of thromboembolic events in patients with chronic AF compliant with recommended dabigatran therapy.2
Results on dabigatran plasma concentrations showed a high inter-individual variation in plasma levels of dabigatran. In a pre-specified analysis of RE-LY, plasma concentrations of dabigatran showed a fivefold variation, and were related to clinical outcomes of ischaemic stroke/ systemic embolism and major bleeding.1 As a result, the use of plasma concentrations for tailoring dabigatran dosing is the subject of on-going discussion.8,9
In our patient we measured a dabigatran value of 35 ng/ ml at six hours after dosing. Assuming a dabigatran half-life of 12-17 hours, a dabigatran trough concentration of approximately 24-27 ng/ml can be expected. Based on the data of Reilly et al.1 this would lead to a median hazard ratio for thrombotic risk of at least 1.5 (confidence interval 1.1-2.2). This illustrated that our patient had a significantly increased risk for ischaemic stroke and systemic embolism, for which increasing the dabigatran dose might be beneficial. Although the dabigatran plasma concentration was low, the impaired renal function and concomitant use of verapamil could have increased the dabigatran plasma concentration in our patient.10 As a result, plasma dabigatran could have been even lower in case of normal renal function and absence of verapamil. In conclusion, we describe a patient with several thromboembolic events under dabigatran 110 mg twice daily treatment with a low dabigatran plasma concentration. This case report shows that in selected patients there might be an indication for dose adjustments based on serum levels of dabigatran to ensure patient efficacy (thromboembolic events) and safety (bleeding). We suggest measurement of dabigatran trough concentration in patients at least once after a steady-state has been reached, approximately after three days, to adjust the dose of dabigatran. More research is warranted.
REFERENCES