KEYWORDS
Aneurysm, vascular graft, chronic Q fever, 18F-FDGPET/ CT, sensitivity, specificity
INTRODUCTION
Q fever is a zoonotic infection caused by Coxiella burnetii, an intracellular and Gram-negative bacterium. C. burnetii is globally present and the reservoir is found in various animals, such as goats, cattle, sheep and household pets. Humans can be infected by inhalation of contaminated aerosols.1 Although often underdiagnosed, Q fever should be considered a public health problem in many countries such as France, Australia, United Kingdom, Italy, Spain, Germany, Israel, Greece and Canada. Q fever often goes unrecognised due to poor surveillance of the disease and the usually asymptomatic infection.1,2 Two clinical forms of Q fever are described: acute Q fever and chronic Q fever. While primary C. burnetii infection is asymptomatic in 60% of all infected persons, the other 40% manifest with a self-limiting flu-like illness known as acute Q fever, which can be complicated by pneumonia or hepatitis.1
Chronic Q fever can develop months to years after primary infection. Patients with a history of cardiac valvulopathy or valvular surgery, an aneurysm or a central vascular graft (central vascular disease), non-haematological malignancy, pregnancy, renal insufficiency or older age are at risk of developing chronic Q fever.3,4 Generally, 1-5% of all patients infected with Coxiella burnetii will develop chronic Q fever.4,5
Recently, we reported a study in which a large population of patients with central vascular disease were screened in a Q fever epidemic area in North-East Brabant, the Netherlands. A total of 16.8% of patients showed evidence of Q fever infection, of which 30.8% fulfilled the criteria of a chronic Q fever infection (in the context of central vascular disease, these infections could be considered what is referred to in the French literature as ‘vascular’ chronic Q fever).6 These figures suggest that the rate of development to chronic Q fever among patients with central vascular disease is high. Chronic Q fever in patients with central vascular disease often manifests as a mycotic aneurysm or an infected vascular graft. These infections can be accompanied by life-threatening complications such as a ruptured aneurysm, aorta-enteric fistula, aorta-caval fistula and spondylodiscitis. Mortality rates of 13.3-40% in the absence of antibiotic therapy and surgical intervention have been reported.7-10
Diagnosing chronic Q fever is still challenging. The Dutch Q Fever Consensus Group published a diagnostic guideline based on the available literature and clinical experience, in which the probability of a patient having chronic Q fever is defined using serology, polymerase chain reaction (PCR) results in blood/tissue, clinical parameters, pathology and imaging studies, such as ultrasound, magnetic resonance imaging (MRI), computed tomography (CT) and 2-deoxy-2-[18F]fluoro-D-glucose positron emission tomography/computed tomography (18F-FDG PET/CT). The guideline categorises chronic Q fever patients as having proven, probable or possible disease.11 Thus far, no real gold standard for the diagnosis of chronic Q fever is at hand. According to the Dutch consensus guideline, proven chronic Q fever is diagnosed if PCR for C. burnetii DNA is positive in blood or tissue, in the absence of acute Q fever infection, or in case of a patient with central vascular disease and a serological profile of chronic Q fever (IgG phase I titre ≥ 1:1024) and if large vessel or prosthetic infection is suggested by imaging (18F-FDG PET/CT, CT, MRI or cardiac ultrasound). Probable chronic Q fever in patients with central vascular disease is diagnosed in case of a serological profile of chronic Q fever without a positive PCR or signs of infection by imaging.11 Analysis of patients in the National Chronic Q Fever Database showed positive PCRs in the blood of only 44% of the patients with chronic Q fever.12
A recent study into the diagnostic performance of serology using the 1:1024 cut-off titre for IgG phase I revealed high sensitivity but low specificity for diagnosing proven chronic Q fever.13,14 PCR for C. burnetii DNA in blood samples has a sensitivity of 50-70%, but a specificity of 100%.1,13,14 The combination of outcomes of serology and PCR tests in blood is considered to provide the best reliable diagnostic criteria for chronic Q fever. 18F-FDG PET/CT is included in the Dutch consensus guideline based on reports describing it as a promising tool for diagnosing infected aortic grafts and/or mycotic aneurysms. In patients with these conditions, 18F-FDG PET/CT demonstrated a good diagnostic performance with a sensitivity of 91-93% and a specificity of 70-95%.15-22 Additionally, 18F-FDG PET/CT is a proven technique used in the work-up of patients with fever of unknown origin.23 In the Dutch guideline for chronic Q fever, 18F-FDG PET/CT is one of the imaging modalities proposed to identify a focus for infection. However, the value of 18F-FDG PET/CT in this selected group of chronic Q fever patients is not yet well established. In 2013, Barten et al. reported an article in which 18F-FDG PET/CT showed a focus of infection in 10 out of 13 patients with proven chronic Q fever (Q fever endocarditis and ‘vascular’ chronic Q fever), concluding that 18F-FDG PET/CT is a helpful imaging technique for localising the infection site of chronic Q fever.24 Furthermore, in the literature, two case reports describing the use of 18F-FDG PET/CT in diagnosing an infected vascular graft in patients with chronic Q fever were published, both advising to use 18F-FDG PET/CT in these patients.25,26
The aim of this study is to describe the single value of 18F-FDG PET/CT in diagnosing chronic Q fever in patients with central vascular disease and evaluating the added value of 18F-FDG PET/CT in the combination strategy in the Dutch consensus guideline. Therefore, we addressed the question how often 18F-FDG PET/CT detects a vascular focus in patients with central vascular disease and proven chronic Q fever.
MATERIAL AND METHODS
Patients
From November 2009 to May 2012, all chronic Q fever patients with an aneurysm of the central arteries or a central vascular graft (abdominal aortic aneurysm (aorta ≥ 30 mm), aneurysm of the common iliac artery (> 12 mm) or aorto-iliac reconstruction, such as an endovascular aneurysm repair or open aorto-iliac reconstruction) and an IgG phase I titre ≥ 1:1024 were included in a multidisciplinary treatment program in the Jeroen Bosch Hospital in ’s-Hertogenbosch and Bernhoven Hospital in Uden, the Netherlands. Within this program, 18F-FDG PET/CT and transthoracic cardiac ultrasound were performed to identify a focus for infection. Patients were partly retrospectively included and partly prospectively.
Patients were included in the PCR-positive study group if diagnosed with an IgG phase I titre ≥ 1:1024 and a positive PCR in blood or tissue; this combination of diagnostic criteria is considered the gold standard for proven chronic Q fever according to the Dutch consensus guideline. The PCR-negative study group included patients with an aneurysm of the central arteries or a central vascular graft and an IgG phase I titre ≥ 1:1024 but a negative PCR for C. burnetii DNA in blood and/or tissue. In these two patient groups, 18F-FDG PET/CT was performed before starting any antibiotic treatment.
The control group consisted of patients with an aneurysm or a central vascular reconstruction and a negative serological profile for Q fever, in whom 18F-FDG PET/CT was performed to evaluate an illness other than an infected aneurysm or vascular graft, with normal white blood cell (WBC) count and C-reactive protein (CRP) level.
Microbiological procedures
Sera were tested for C. burnetii antibodies using immunofluorescence assay (IFA, Focus Diagnostics, Inc., Cypress, CA, USA), assessing the presence of IgM and IgG antibodies to phase I and II antigens. If the IgG phase I titre was ≥ 1:512, sera were also tested by PCR for the presence of C. burnetii DNA. The NucliSensEasyMAG extraction system (bioMerieux, Boxtel, the Netherlands) was used for extraction of DNA from serum and/or tissue. PCR was performed as previously described.27
18F-FDG PET/CT
All 18F-FDG PET/CT scans were performed at the Department of Nuclear Medicine of the Jeroen Bosch Hospital, which is accredited by European Association of Nuclear Medicine Research Ltd. 18F-FDG PET/CT was performed according to the European Association of Nuclear Medicine procedure guidelines.28 Patients fasted for at least six hours before injection of 18F-FDG. A dose of 4.5 MBq per kg was injected 60 min before the start of the scan. Scans were performed on a Biographm CT or Biograph 16 scanner (Siemens Medical Systems, Knoxville, TN, USA) scanning three minutes per bed position from the base of the skull to the middle of the femora. Covering the same area, low-dose CT was performed for attenuation correction. Data were reconstructed in three dimensions. PET, CT and fused images were reviewed using Syngovia software (Siemens). 18F-FDG PET/CT scans were interpreted independently by two experienced nuclear physicians, aware of the suspicion of chronic Q fever. Scans were analysed using a visual grading scale in combination with the pattern of 18F-FDG uptake as described in table 1. 9,18 In case of disagreement, a third reader was consulted and a final conclusion was made after a consensus meeting.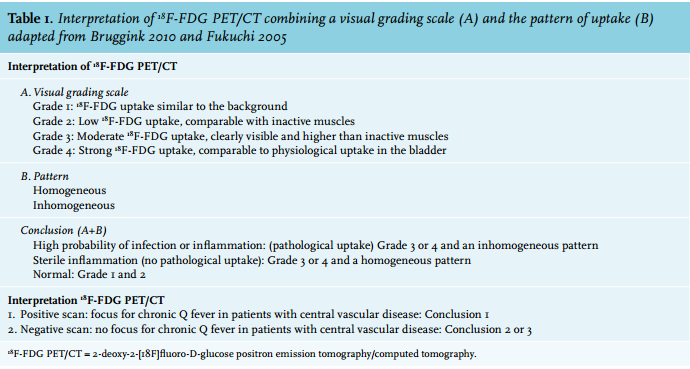
Infection parameters
WBC counts and CRP levels were retrieved from the hospital information system and compared for patients with a positive or negative 18F-FDG PET/CT in the PCR-positive and PCR-negative Q fever study groups.
Clinical outcome
The clinical outcome in terms of cure was evaluated within the PCR-positive and the PCR-negative study groups between patients with a positive and negative 18F-FDG PET/ CT. Patients were considered cured if the IgG phase I titre reached < 1:1024. A favourable treatment response was defined as a fourfold or higher IgG phase I titre decrease with no or minimal clinical complaints.
Data analysis
Results of 18F-FDG PET/CT in the PCR-positive patient group (gold standard) were compared with results in the control group to assess the diagnostic performance of 18F-FDG PET/CT in finding a vascular focus for chronic Q fever. Within the PCR-negative group, 18F-FDG PET/ CT results were compared with those in the PCR-positive group. The diagnostic performance was expressed in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) with Wilson 95% confidence intervals (CI). Mean WBC counts and CRP levels with standard deviations and p-values (Fisher’s exact test and the single Chi-square test) were calculated using SPSS 18.0 (SPSS Inc., Chicago, IL, USA).
The study protocol is registered in Clinicaltrial.gov, a protocol registration system (registration number: NCT01450501 ID: 50-51800-98-013). The study was ethically approved by the local feasibility committees of the Jeroen Bosch Hospital and Bernhoven Hospital; approval of a regional Medical Research Ethics Committee was not necessary for this study as patients were treated according to the Dutch consensus guideline.
RESULTS
PCR-positive study group
Between November 2009 and May 2012, 13 patients were included in the PCR-positive study group and 22 in the control group. In three of the 13 patients in the PCR-positive study group, chronic Q fever infection was diagnosed by a positive PCR on tissue samples of the vascular wall, while ten patients were included due to positive PCR in blood. Transthoracic echocardiography was performed in all patients and none of them had signs of endocarditis. No abscesses or signs of spondylodiscitis were found in these patients with 18F-FDG PET/CT. None of the patients included in this report were taking any medication such as prednisone, methotrexate, TNF-alpha and rituximab when 18F-FDG PET/CT was performed. Fifty percent of the patients used a statin at the time of diagnosis; no difference was found between patients with or without statin use.
While reviewing the 18F-FDG PET/CT scans, a third reader was consulted for two out of 35 scans (all in the positive-PCR study group); a final conclusion was made after a consensus meeting.
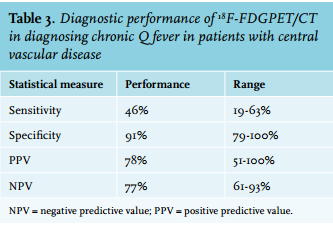
18F-FDG PET/CT indicated pathological vascular uptake in six out of 13 (46%) patients in the PCR-positive study group, while no pathological uptake or a sterile inflammation was observed in three and four patients, respectively (as shown in figure 1). In the control group, 18F-FDG PET/ CT showed pathological vascular uptake in two out of 22 (9%) patients. One of the positive patients had undergone endovascular aneurysm repair in 2003, while the other one had received an aortic graft in 2006. Follow-up after 72 and 108 months (solely based on clinical follow-up, no second 18F-FDG PET/CT was performed), respectively, revealed no signs of an infected graft (table 2). In the remaining 20 patients, no pathological uptake was observed in nine patients (one patient with a central graft and eight patients with an aneurysm), while eleven patients showed signs of a sterile inflammation (four patients with a central graft and seven patients with an aneurysm). 18F-FDG PET/CT has a sensitivity of 46% (95% CI: 23-71%), specificity of 91% (95% CI: 71-99%), PPV of 75% (95% CI: 41-93%) and NPV of 74% (95% CI: 55-87%) for detecting chronic Q fever in patients with central vascular disease (table 3). Two of the three patients with a positive C. burnetii PCR of the vascular wall showed a positive 18F-FDG PET/CT.
We checked for differences in uptake (especially a difference in homogeneous and heterogeneous uptake) between patients with an aneurysm or graft (table 4). No differences were found and therefore we decided it is valid to combine the two groups (p = 0.169). Additionally, the distribution in the pattern of uptake is distinctly different in the grade 1/2 and grade 3/4 group. In grade 3/4 a clear difference in distribution of pattern of uptake is seen between the PCR-positive group and the control group.
Table 5 shows the mean WBC count and CRP level in patients in the PCR-positive study group with a positive 18F-FDG PET/CT compared with patients with a negative 18F-FDG PET/CT. No significant differences were observed (p = 0.434 and p = 0.640, respectively).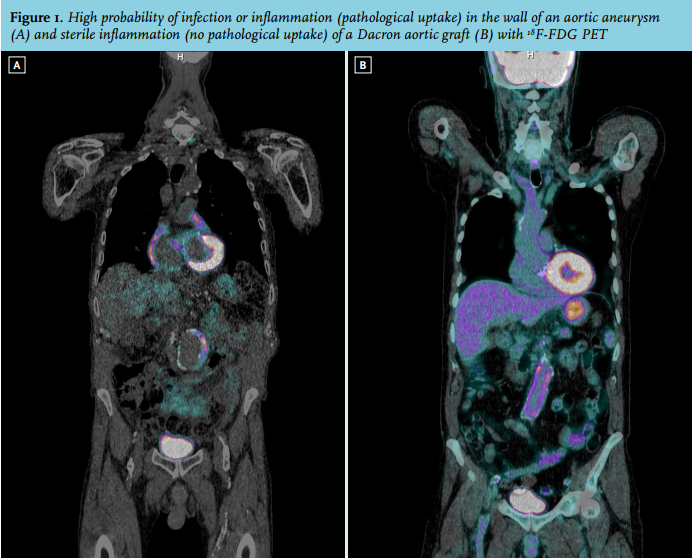

PCR-negative study group
Twenty patients were evaluated in the PCR-negative study group. 18F-FDG PET/CT showed pathological vascular uptake in ten out of 20 (50%) patients. In the remaining ten patients, no pathological uptake was observed in five cases, while 18F-FDG PET/CT was indicative of a sterile inflammation in the other five patients. The percentage of positive 18F-FDG PET/CT scans within the PCR-positive group did not differ from the number of positive 18F-FDG PET/CT scans in the PCR-negative group (46% versus 50%). Additionally, one patient without pathological uptake of 18F-FDG on PET/CT within the PCR-negative group subsequently underwent surgery (after closure of the study) and the vascular wall tissue was found to be C. burnetii PCR positive. In the PCR-negative study group, infection parameters were low in patients with a positive 18F-FDG PET/CT as well as in patients with a negative 18F-FDG PET/CT without significant differences (see table 5).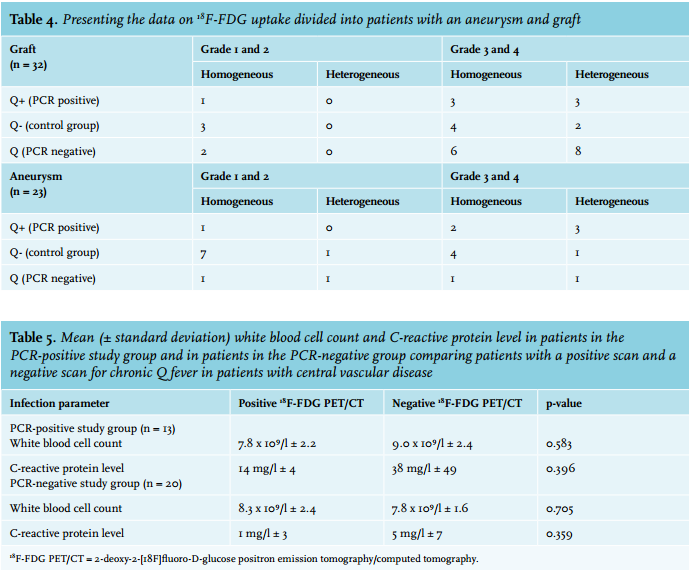
DISCUSSION
Considering the high morbidity and mortality in patients with chronic Q fever and central vascular disease, diagnosing the disease is key to starting early treatment and preventing complications. In the Dutch consensus guideline for diagnosing chronic Q fever, 18F-FDG PET/ CT is listed as one of the imaging tools available to identify a focus of infection. Previous literature concluded that 18F-FDG PET/CT is a helpful imaging technique for localising the infection site caused by a chronic Q fever infection.24 Furthermore, 18F-FDG PET/CT is a valuable imaging tool to identify a vascular prosthesis infection with a sensitivity ranging from 91-93% and a specificity of 70-95%.7,9,18 When scans are visually analysed, combining a grading scale with the pattern of 18F-FDG uptake, the specificity significantly improved from 70 to 95% as shown in a study by Fukuchi et al.9 This method was also applied in this study and a difference in distribution of pattern of uptake (homogeneous or heterogeneous) was seen between the PCR-positive group and control group implying that the pattern of uptake is of added value. However, a differentiation between inflammation and infection cannot be made with 18F-FDG, as is mentioned in table 1. Although the specificity of 91% that we observed is in line with the results of Fukuchi et al., a much lower sensitivity was observed in our PCR-positive study group with proven chronic Q fever patients and central vascular disease.
The explanation for the observed low sensitivity is not clear. As a result of increased glycolytic activity, inflammatory cells (neutrophils and macrophages) as well as tumour cells show increased uptake of 18F-FDG at sites of inflammation, infection and malignancy.29 One report by Lepidi et al. described a histopathological quantitative analysis on infiltrating cells comparing the valve tissue of patients with Q fever endocarditis to non-Q fever-infected valve tissue.30 It was demonstrated in this study that valve tissue damaged by chronic Q fever infection was localised in different parts of the valve and often concerned small and discrete regions.29 If such discrete changes are also present in chronic Q fever with a vascular focus, this could be an explanation for the low sensitivity of 18F-FDG PET/ CT in the PCR-positive study group. Further research, especially on histopathology of the vascular tissue, is needed to confirm this hypothesis. Recently, we published a report concerning the histopathology of the vascular wall in patients with chronic Q fever with a vascular focus in which we demonstrated a necrotising granulomatous infiltration response in only four out of seven patients. Unfortunately, the number of patients was too small to correlate with the results of the 18F-FDG PET/CT.31
In the Dutch consensus guideline, proven chronic Q fever in patients with central vascular disease is diagnosed either by PCR positivity or through the combination of a serological profile matching chronic Q fever and proven large vessel or prosthetic infection by imaging studies such as 18F-FDG PET/CT.11 As the IgG phase I cut-off titre of ≥ 1:1024 has a sensitivity of 97.8% and a specificity of < 21.4% for diagnosing proven chronic Q fever, an imaging test with a high specificity would be beneficial for the diagnostic strategy presented in the Dutch consensus guideline.11 Due to the high specificity of the 18F-FDG PET/CT observed in this report (91%), we think it is acceptable to categorise patients with central vascular disease, an IgG phase I titre ≥ 1:1024 (high sensitivity) and a positive 18F-FDG PET/CT (high specificity) as having proven chronic Q fever, as recommended in the Dutch consensus guideline. PCR-negative patients with central vascular disease, an IgG phase I titre ≥ 1:1024 and a negative 18F-FDG PET/CT are classified as having probable chronic Q fever. Long-term antibiotic treatment and optional surgical intervention in patients with central vascular disease and proven chronic Q fever is advised.32,33 Treatment of a patient with probable chronic Q fever and central vascular disease is more debatable and depends on the possible advantages and disadvantages of this treatment for the individual patient. In clinical practice, however, most patients with probable chronic Q fever in the Netherlands are treated with antimicrobial therapy in view of the risk of acute complications and mortality.6,34
In contrast to previous reports, in the wake of the 2007-2010 Dutch Q fever epidemic, a vascular focus of infection (57%) was more often found than an endocarditis focus (35%) among 215 patients with proven and probable chronic Q fever, while imaging studies revealed that the focus of infection may have been both heart valves and vascular structures in only 11 chronic Q fever patients. It is therefore not surprising that endocarditis was absent in our group of Dutch chronic Q fever patients with a vascular infection focus.12
After closure of the study, one patient with a serological profile of chronic Q fever (IgG phase I titre = 1:4096), a negative PCR in blood and negative 18F-FDG PET/CT, underwent surgery and the vascular wall tissue was found to be positive for C. burnetii DNA by PCR. This emphasises the questionable value of both a negative 18F-FDG PET/CT and negative PCR in the blood in patients with a known risk factor and a positive serological profile for chronic Q fever. The fact that a similar number of 18F-FDG PET/CT positive results in the PCR-negative group (ten out of 20) was observed compared with the PCR-positive study group (six out of 13) also suggests that PCR in blood lacks sufficient sensitivity in patients with a known risk factor and a positive serological profile for chronic Q fever. The future could bring us more information concerning the diagnostic value of the different tests used in the Dutch consensus guideline. This might result in revision of this guideline, improving the healthcare for patients with chronic Q fever and central vascular disease, provide indications for an early start to treatment and prevent complications.
Limitations of this study are the low number of included patients and the fact that the reviewers of the scans were not blinded for outcome. Another limitation is the lack of a true gold standard for chronic Q fever with a vascular focus. PCR data on vascular tissue were absent in most patients as no surgical treatment or autopsy was performed in 10/13 patients in the PCR-positive group and 0/20 patients in the PCR-negative group.
CONCLUSION
The combination of 18F-FDG PET/CT, as an imaging tool for identifying a focus of infection, and Q fever serology is a valid diagnostic strategy for diagnosing chronic Q fever in patients with central vascular disease.
ACKNOWLEDGEMENTS
This study was financially supported by the Netherlands Organization for Health Research and Development (ZonMw, grant no. 205520001). The sponsor had no involvement in the study design, data collection, data analysis or interpretation of the study results. The authors declare no conflict of interest.
DISCLOSURES
There are no conflicts of interest.
REFERENCES