KEYWORDS
Guillain-Barré syndrome, Takotsubo cardiomyopathy, negative T waves, echocardiography, enoximone
INTRODUCTION
Guillain-Barré syndrome (GBS) is an autoimmune disorder in which autoantibodies affect the peripheral nervous system. Autonomic dysfunction is a common and severe complication of GBS. Various clinical cardiovascular complications in these patients can occur, such as arrhythmias, wide blood pressure fluctuations and even cardiac arrest. Takotsubo cardiomyopathy is a rare complication in GBS. We present a patient with GBS who developed takotsubo cardiomyopathy shortly after admission to the ICU because of respiratory deterioration.
Clinicians should be aware of this potentially lethal complication and the therapeutic options.
CASE REPORT
A 39-year-old female was admitted to the ICU with high fever and respiratory deterioration. She was recently diagnosed with GBS and suffered progressive muscle weakness despite a five-day course of immunoglobulins. Otherwise, she was healthy and was not taking any prescription drugs. On admission to the ICU her heart rate was 90 beats per minute, blood pressure 140/80 mmHg and a temperature of 39 °C.
One hour later intubation was necessary because of progressive respiratory failure due to muscle weakness and mucous plugging. To induce anaesthesia etomidate and rocuronium were used. Shortly after an uncomplicated intubation, a marked increase in heart rate (170-180 beats /min) was noticed and her blood pressure dropped to as low as 85/45 mmHg. Despite fluid loading her blood pressure stayed low. Because of recent immobilisation, the ICU physician on call decided to perform of a computed tomography (CT) scan to rule out pulmonary embolism. It only showed atelectasis of the left lower lobe but no signs of pulmonary embolism. Pneumosepsis with fever, tachycardia and hypotension was then regarded as the most likely diagnosis. In the following hours antibiotics, additional fluids, norepinephrine and hydrocortisone were given. Blood pressure stayed low, tachycardia persisted and urine output ceased. The electrocardiogram revealed a sinus tachycardia with nonspecific ST-T segment changes. Because of the lack of improvement, concomitant heart failure was suspected. Laboratory results showed a normal creatine kinase (56 U/l, normal < 145 U/l), elevated troponin (0.198 µg/l, normal < 0.014 µg/l) and NT-pro-BNP (1391 pmol/l, normal < 15 pmol/l). Thyroid function was normal. Echocardiography showed akinesia of the septum and inferior left ventricular wall, and apical akinesia which could not be explained by regional coronary hypoperfusion. The estimated left ventricular ejection fraction was only 10%. Revision of the CT scan showed no coronary calcification. In a young non-smoking female with no other risk factors for coronary artery disease and no coronary calcifications on the CT scan, coronary angiography was deemed to be an unnecessary risk with a low probability of finding coronary artery disease. Based on the typical findings on echocardiography it was concluded that the patient was suffering from takotsubo cardiomyopathy. Enoximone infusion was started to assist left ventricular contractility and to reduce afterload. This resulted in a gradual increase in blood pressure and return of diuresis. The next day, additional furosemide was given because of a positive fluid balance and signs of pulmonary congestion on the chest X-ray. In the next 48 hours, the enoximone was tapered off. Because her sinus tachycardia persisted metoprolol was introduced stepwise over three days to reduce the sympathetic tone and improve myocardial work/oxygen consumption ratio; the maintenance dose was 50 mg twice a day. Repeat follow-up echocardiography showed gradual normalisation of left ventricular performance in the next four months.
DISCUSSION
We present a patient diagnosed with GBS who developed takotsubo cardiomyopathy. Massive catecholamine release due to the stressful event of rapid respiratory deterioration and haemodynamic instability after induction of anaesthesia most likely caused the development of takotsubo cardiomyopathy. In addition, norepinephrine infusion could have aggravated catecholamine excess which might have contributed to her myocardial dysfunction.
Takotsubo cardiomyopathy can be difficult to distinguish from the more common cardiovascular complications in GBS due to autonomic dysfunction such as tachyarrhythmias and bradyarrhythmias, blood pressure fluctuations, acute coronary syndromes and myocarditis.1
The name Takotsubo refers to a Japanese jar used by fishermen to catch octopuses. The round bottom but tight neck resemble a picture often seen at echocardiography of the left ventricular wall, called apical ballooning. As more reports were published, it became clear that wall movement disorders were not restricted to the apex but could involve multiple segments of the left ventricular wall.2 The Mayo Clinic proposed criteria for takotsubo cardiomyopathy: (A) transient hypokinesis, akinesis, or dyskinesis in the mid segments of the left ventricular wall with or without apical involvement; regional wall motion abnormalities not related to one coronary supply region; frequently, but not always, a stressful trigger is present; (B) absence of obstructive coronary artery disease or angiographic evidence of plaque rupture; (C) new ECG abnormalities (ST elevation or T wave inversion) and (D) absence of myocarditis or pheochromocytoma.3 Recently, Madias argued that these criteria have been outpaced by the rapidly accumulating clinical experience, and thus need to be replaced by more realistic sets of diagnostic rules.4
The exact pathogenic mechanism of takotsubo cardiomyopathy is still controversial. The catecholamine hypothesis, commonly induced by physical and/or emotional stress, seems the best explanation.5 Sympathetic excitation of the brain triggers the release of the catecholamines norepinephrine and epinephrine, resulting in hyperdynamic basal contraction and apical systolic dysfunction. Takotsubo cardiomyopathy is a specific type of a broad spectrum of reversible cardiomyopathies,6,7 often stress related. The association of GBS with stress cardiomyopathy is not well understood. Dysregulation of autonomic tone with excessive sympathetic activation in GBS with elevated catecholamines levels has been reported.8,9 Also in subarachnoid haemorrhage, traumatic brain injury and other neurological emergencies, excessive catecholamine release secondary to the primary insult has been reported, causing what is known as neurogenic stress cardiomyopathy.9
To our knowledge eight case reports associating GBS and takotsubo cardiomyopathy have been reported in the literature.10-17 In our review of the literature ECG changes (negative T waves) were present in all but one patient. Takotsubo cardiomyopathy presented within the first week of hospital admission and three patients required mechanical ventilation. Treatment consisted of angiotensin-converting enzyme inhibitors (ACE), β-blockers, digoxin and diuretics (table 1). One patient needed dopamine infusion for cardiac support. Our patient was successfully treated with enoximone, a phosphodiesterase inhibitor which has positive inotropic as well as vasodilating properties and therefore reduces afterload. Later, she was given a β-blocker. Although the mode of action of β-blockers in heart failure is still incompletely understood, they are believed to reduce sympathetic tone and improve the myocardial work/oxygen consumption ratio, among other things.18
Treatment must be individualised for each patient. The use of norepinephrine in this light may be counterproductive. We chose to use enoximone instead of dopamine or dobutamine because of her tachycardia.
Beta-blockade seems sensible in case of dynamic mid-ventricular obstruction, represented by a high intraventricular pressure gradient on echocardiography.19 ACE inhibition may be used to reduce afterload in haemodynamically stable patients.
Takotsubo cardiomyopathy should be considered in GBS when ECG abnormalities are present. The easiest way to do this is to perform echocardiography. According to the Mayo Clinic guidelines, acute coronary disease and myocarditis should be ruled out when suspected. In our case coronary artery disease was regarded as unlikely because of her young age, absence of risk factors for coronary artery disease and normal creatine kinase. Furthermore, electrocardiography and cardiac ultrasound showed abnormalities that could not be explained by regional coronary hypoperfusion/ischaemia while retrospective analysis of a CT scan showed no coronary calcifications. 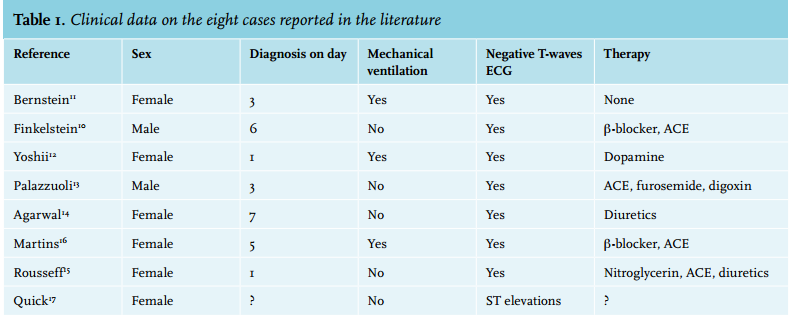
CONCLUSION
We report a case of severe takotsubo cardiomyopathy, which required prompt management in terms of diagnostics and treatment. Takotsubo cardiomyopathy is a rare complication during the acute phase of GBS and must be distinguished from autonomic dysfunction. Especially ECG abnormalities such as negative T waves should alert the clinician to the presence of takotsubo cardiomyopathy.
DISCLOSURES
The authors declare no conflict of interest. No funding or financial support was received.
REFERENCES