KEYWORDS
Acute renal failure, drug interactions, rhabdomyolysis
BACKGROUND
The Guidelines of the European Society of Cardiology (ESC) advise the use of antiplatelet agents inhibiting signal transduction to the platelet P2Y12 adenosine diphosphate receptor (ADP) in patients with acute coronary syndrome (ACS).1,2
Ticagrelor is a new, oral P2Y12 adenosine diphosphate receptor antagonist. Ticagrelor is metabolised by CYP3A4; 58% of ticagrelor is excreted in the faeces, and 27% in the urine, predominantly as inactive metabolites.3 Unlike clopidogrel and prasugrel, ticagrelor binds reversibly to the receptor. Both the parent drug and first metabolite, with elimination half-lives of 7 and 9 hours respectively, have antiplatelet activity.4 These specific properties allow a relatively rapid onset of action. The PLATelet inhibition and patient Outcomes (PLATO) trial showed that ticagrelor significantly reduced the rate of death from cardiovascular events in patients with ACS as compared with clopidogrel, regardless of renal function.5 Patients with chronic kidney disease have a poorer responsiveness to clopidogrel treatment.6,7 Subgroup analysis of the PLATO trial showed that the benefits of ticagrelor over clopidogrel are larger in patients with impaired renal function.8 Based on the PLATO trial5 it is now strongly recommended by the ESC to prescribe ticagrelor (loading dose 180 mg orally followed by a maintenance dose of 90 mg twice daily) for all patients at moderate-to-high risk regardless initial treatment strategies.1
Combined prescription of ticagrelor and statins is common. Statins are notorious for causing rhabdomyolysis. Risk increases with higher doses or interactions with other medicaments.9 Both simvastatin and ticagrelor are metabolised by CYP3A4. Ticagrelor is a weak inhibitor of CYP3A4. Combined prescription will result in higher serum concentrations of simvastatin, potentially evoking rhabdomyolysis. The prescribing information of ticagrelor recommends to avoid simvastatin doses over 40 mg.4 In contrast to simvastatin, rosuvastatin, which was used in this case, is not metabolised by CYP3A4.10 However, dosage of rosuvastatin should be adjusted in patients with renal failure, since its plasma levels may increase threefold with an eGFR < 30 ml/min. Therefore, doses over 40 mg daily are contraindicated in patients with moderate renal impairment (< 60 ml/min). The use of rosuvastatin in patients with severe renal impairment (< 30 ml/min) is contraindicated for all doses.11
In the World Health Organisation (WHO) Adverse Drug Reaction Database, rhabdomyolysis was registered 17 times as adverse reaction of ticagrelor; in all cases the patient used a statin.
CASE PRESENTATION
A 78-year-old man was referred to the emergency department with acute renal failure. The medical history revealed hypercholesterolaemia and two myocardial infarctions, the second one month before admission. The patient had been nauseous and vomiting for six days. He complained about myalgia and muscle cramps. Medication included perindopril 2 mg twice daily, amlodipine 5 mg once daily, metoprolol 25 mg twice daily, omeprazole 20 mg once daily, rosuvastatin 40 mg once daily, ezetimibe 10 mg once daily and ticagrelor 90 mg twice daily. His blood pressure was 146/87 mmHg and pulse rate 89 beats/min.
Physical examination revealed no abnormalities, except pain upon palpation of the calves. Initial laboratory testing showed a serum creatinine of 674 µmol/l (one month previously this was 108 µmol/l), eGFR of 10 ml/min, serum urea of 25.7 µmol/l and creatinine kinase (CK) of 10,872 IU/l. The urine sediment revealed leukocytes (++), red cells (+++) and proteinuria (3.1 g/24 hours). It is a well-known fact that red cells in qualitative urine analysis can be caused by the presence of free haemoglobin or myoglobin. The working diagnosis was acute renal failure due to rhabdomyolysis and dehydration due to vomiting, aggravated by use of an ACE inhibitor in a dehydrated state. Treatment with infusion of physiological saline solution and bicarbonate was started. Rosuvastatin (the assumed cause of rhabdomyolysis), perindopril and amlodipine were discontinued.
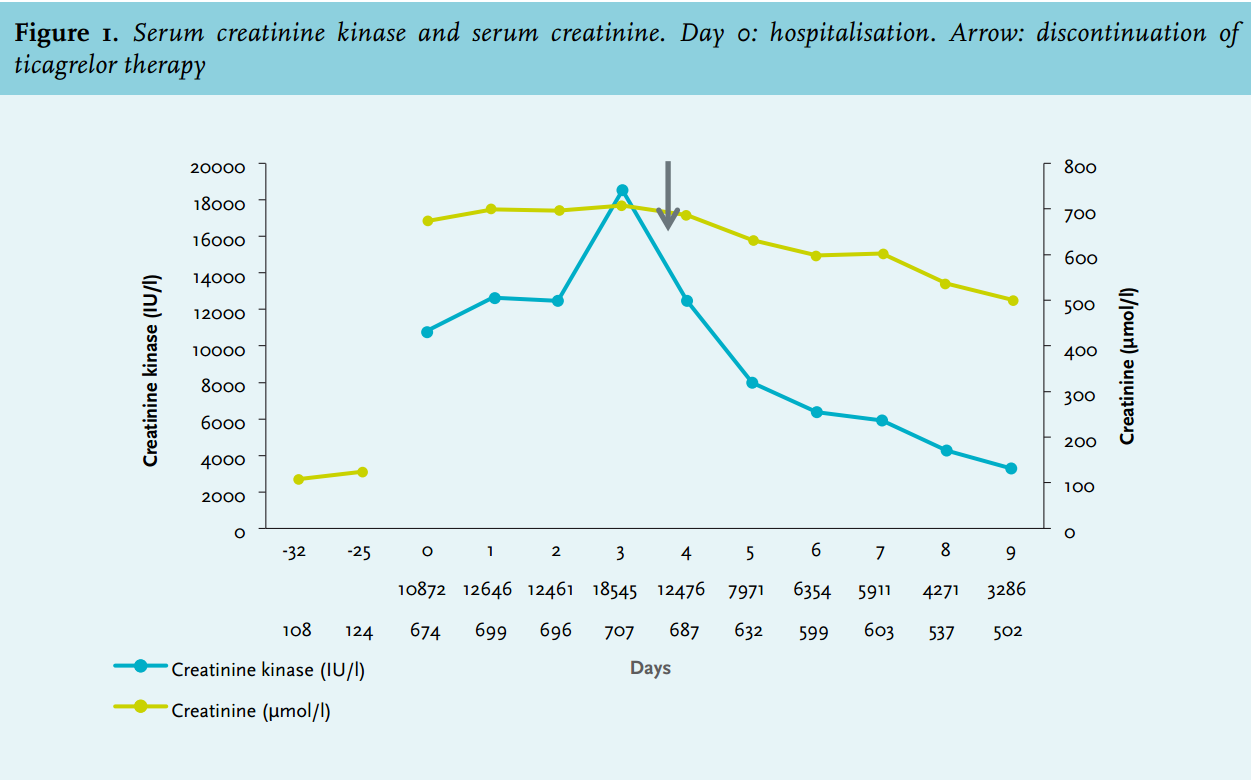
Clinical symptoms remained unchanged over the next four days and the serum CK rose further to 18,545 IU/l and the creatinine concentration to 707 µmol/l. The diagnosis was reconsidered: rosuvastatin and ezetimibe had been used in the current dosage for six years without symptoms. The only recent change in medication was the start of ticagrelor one month earlier, suggesting a role for ticagrelor in the rhabdomyolysis. Ticagrelor was discontinued, as were omeprazole and ezetimibe. From that moment on (day 4) the patient recovered and serum creatinine and CK values decreased gradually (figure 1). At the moment of discharge from the hospital the serum concentration of CK was 3286 IU/l and the serum creatinine concentration was 502 µmol/l. In retrospect, one week after the start of ticagrelor, the serum creatinine had risen from 108 µmol/l (eGFR 60 ml/min) up to 124 µmol/l (eGFR 52 ml/min).
DISCUSSION
In the PLATO trial, serum creatinine concentration significantly increased by more than 30% in 25.5% of the patients receiving ticagrelor. In 8.3% of these patients creatinine levels increased more than 50%. Elevations of more than 50% were more pronounced in patients over 75 years (13.6%), in patients with pre-existent renal impairment (17.8%) and in patients receiving treatment with angiotensin type II receptor inhibitors (11.2%).3,12
The European Medicines Agency recommends to check renal function one month after starting ticagrelor; special attention should be paid to patients with additional risk factors.3 The mechanism leading to an increase in creatinine concentrations is unknown. Ticagrelor prolongs the half-life of adenosine and increases its plasma concentration by inhibition of cellular uptake. Adenosine interferes with the tubuloglomerular feedback system and directly influences renal vascular tone. Adenosine and angiotensin II act synergistically to increase renal vascular resistance and decrease renal blood flow.13-16
In contrast with the reports in the WHO database, rhabdomyolysis does not seem to be a side effect of ticagrelor. Here, it is plausible that ticagrelor led to a deterioration of renal function, resulting in accumulation of rosuvastatin, which provoked rhabdomyolysis. Simultaneous use of ezetimibe was possibly an additional risk factor.10 Serum CK levels declined four days after discontinuation of rosuvastatin, corresponding with the elimination time of rosuvastatin.
Unfortunately, in this patient with multiple risk factors, renal function was not checked one month after initiation of ticagrelor therapy. Additionally, the rosuvastatin dose was not adjusted for the pre-existing mild renal impairment.
ACKNOWLEDGEMENTS
We thank F.T.M. Huysmans, MD, PhD for his critical comments on the manuscript.
DISCLOSURES
The authors declare no conflicts of interest.
REFERENCES